Ectopic Pregnancy: Diagnostic Role of Transvaginal Ultrasound
Introduction
Ectopic pregnancy is the implantation of a fertilized ovum outside the uterine cavity, occurring in about 1–2% of all pregnancies[1].
The fallopian tube is the most common site, particularly the ampullary region, although ovarian, cervical, interstitial, and abdominal locations are also reported[1,5]. It remains a major cause of maternal morbidity and mortality in the first trimester.
Risk factors include previous ectopic pregnancy, tubal surgery, pelvic inflammatory disease, infertility treatments, intrauterine device (IUD) use, and smoking, though many cases present without identifiable risks. Clinical symptoms may range from mild abdominal pain and vaginal spotting to acute abdominal pain and hemodynamic instability in ruptured cases[6].
Diagnosis relies on a combination of serum β-hCG measurement and transvaginal ultrasound (TVUS), which is the imaging modality of choice. Typical ultrasound findings include the absence of an intrauterine pregnancy when β-hCG exceeds the discriminatory zone, an adnexal mass, or an extrauterine gestational sac with or without cardiac activity[4].
Early recognition is essential to guide management, which may be expectant, medical with methotrexate, or surgical, depending on patient stability and clinical findings[2,3,4,5].

Clinical Case
A 31-year-old woman, gravida 0 para 0, presented with complaints of lower abdominal pain and vaginal spotting. She had no history of previous pregnancies or significant medical or surgical conditions. Her last menstrual period (LMP) was April 17, 2025.
She reported experiencing sharp, one-sided lower abdominal pain that began on June 11, 2025, associated with mild vaginal bleeding. She denied any history of trauma, fever, or gastrointestinal symptoms.
On physical examination, the patient was hemodynamically stable. Abdominal palpation revealed localized tenderness in the lower quadrant, with no evidence of peritoneal irritation.
Initial investigations included a urine pregnancy test, which returned positive. Transvaginal ultrasound was performed, revealing an anteverted, non-gravid uterus with no abnormal myometrial shadowing. The endometrium measured 14.2 mm.



Imaging Technique
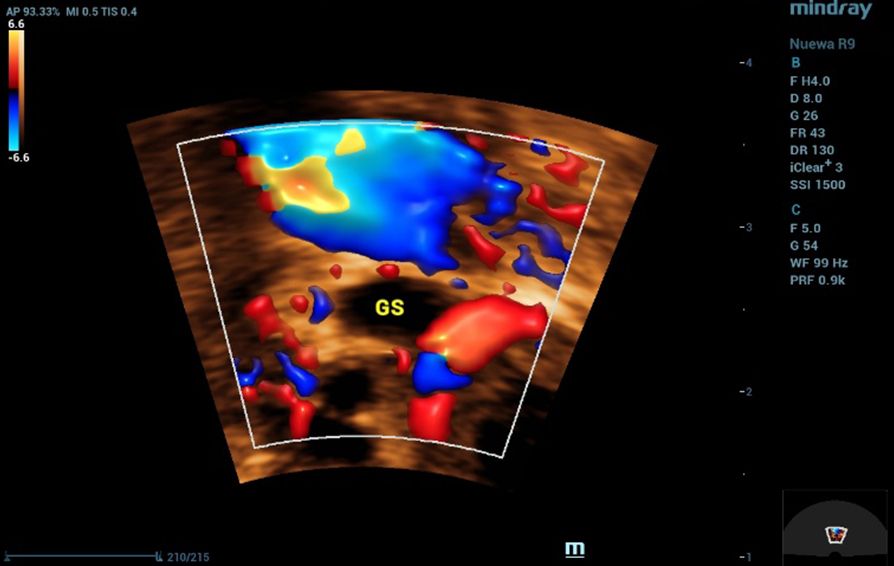
All ultrasound examinations were performed using the Nuewa R9 Ultrasound System (Mindray, Shenzhen, China). A convex transducer (SC6-1U) was employed for general pelvic evaluation, and a 4D transvaginal transducer (DE11-3WU) was used for detailed assessment of the uterus and adnexa. Imaging modalities included two-dimensional (2D) grayscale ultrasound, Color Doppler, and four-dimensional (4D) imaging.
To enhance diagnostic accuracy, advanced imaging applications were applied. Smart Endometrial Receptivity Analysis (Smart ERA) was utilized to assess endometrial morphology and volume, while the SCV+ function was employed to improve spatial resolution and delineation of adnexal structures. These features contributed to the precise characterization of the ectopic gestational sac and detailed evaluation of ovarian and endometrial parameters.
Discussion
Ectopic pregnancy, though occurring in only 1–2% of pregnancies, is a leading cause of first-trimester maternal morbidity and mortality due to its variable presentation and risk of rupture. Early diagnosis is essential to preserve fertility and prevent complications[1].
In this case, transvaginal ultrasound was central to the diagnosis. The examination revealed the absence of an intrauterine gestational sac despite a positive pregnancy test, a finding highly suggestive of ectopic pregnancy. Additionally, a small gestational sac was visualized outside the uterine cavity, confirming the diagnosis. These ultrasound findings, when correlated with the patient’s symptoms of abdominal pain and vaginal spotting, highlight the critical role of transvaginal imaging in detecting ectopic pregnancies at an early stage, enabling prompt intervention and reducing the risk of complications.
References
- Barnhart KT. Clinical Practice. Ectopic Pregnancy[J]. New England Journal of Medicine, 2009, 361(4):379-387.
- Jensen JR, et al. Predictors of Success of Methotrexate Treatment in Women with Tubal Ectopic Pregnancies[J]. New England Journal of Medicine, 1999, 340(10):861-867.
- Gary H. Lipscomb, M.D., Thomas G. Stovall, M.D., and Frank W. Ling, M.D. Nonsurgical Treatment of Ectopic Pregnancy[J]. New England Journal of Medicine, 2000, 343 (18):1325-1329.
- Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester[J]. N Engl J Med. 2013 Oct 10;369(15):1443-51.
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology[J]. ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy. Obstet Gynecol. 2018 Mar;131(3):e91-e103.
- Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review[J]. Am J Obstet Gynecol. 2012 Jul;207(1):14-29.