Basic Information
Authored By: Zhongshan Gou from Dept. U.S.
Hospital Name: The Affiliated Suzhou Hospital of Nanjing Medical University
Instruments and Methods:
- Mindray Resona 8
- Probe D8-2U
- A supine or lateral position should be taken
- Routine obstetric scanning should be performed before the echocardiography exam to exclude extracardiac anomalies
Case Introduction
Patient History:
- Female
- Age 27
- G2P1
- Gestational period 24W3D
Complaint:
Punctate hyperechoic in fetal left ventricular(LV)

Ultrasound Findings:
- The heart is located in the left chest and apex pointing to the left, CTR 0.27.
- Concordant atrioventricular connection. Normal ratio of left and right atrium diameter, a little hyperechoic in the LV. Normal shape and function of atrioventricular valve.
- The consistent connection between ventricle and a great artery .Normal original and size of aorta and pulmonary artery, blood flow unobstructed. Normal Semilunar valve shape and function.
- Normal course and diameter of ductus arteriosus and aortic arch, and unobstructed blood flow.
- The superior and inferior vena cava return to the right atrium, and one pulmonary vein return to the left atrium.
- Normal fetal heart rhythm, HR 142 bpm.
By now, everything is normal. The preliminary diagnosis suggested no significant abnormality in fetal heart structure at present. However, when the probe is slightly tilted from the standard four chamber view to the fetal foot side, the problem occurs:
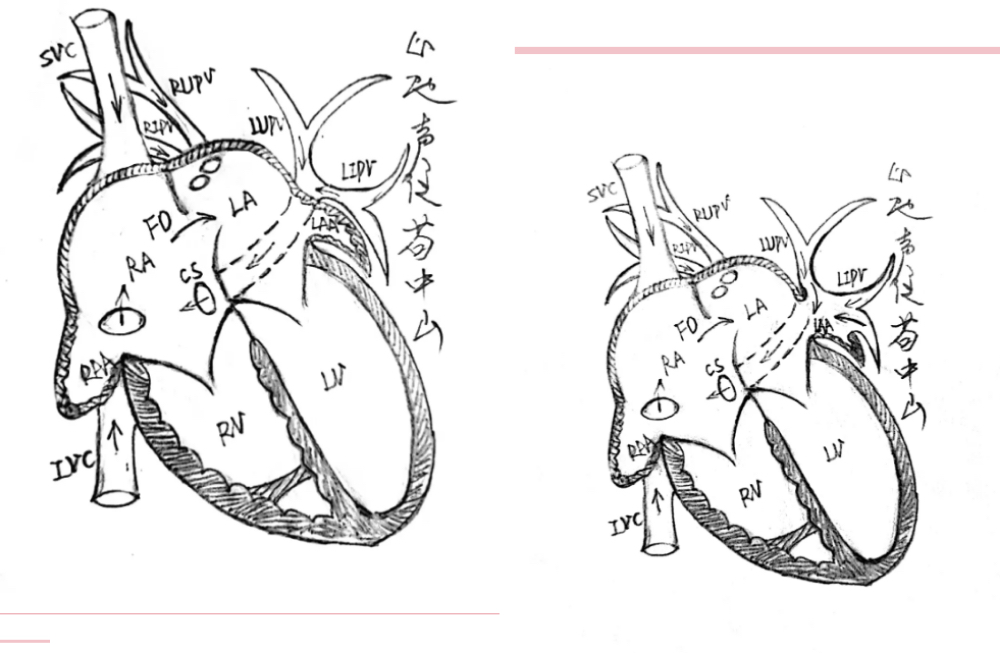
Accordingly, it should be diagnosed as partial anomalous pulmonary venous return (PAPVR, Type II). Intracardiac: left superior pulmonary veins(LSPV) and Left inferior pulmonary vein(LIPV) return to coronary sinus (PAPVR to CS).
Image Analysis
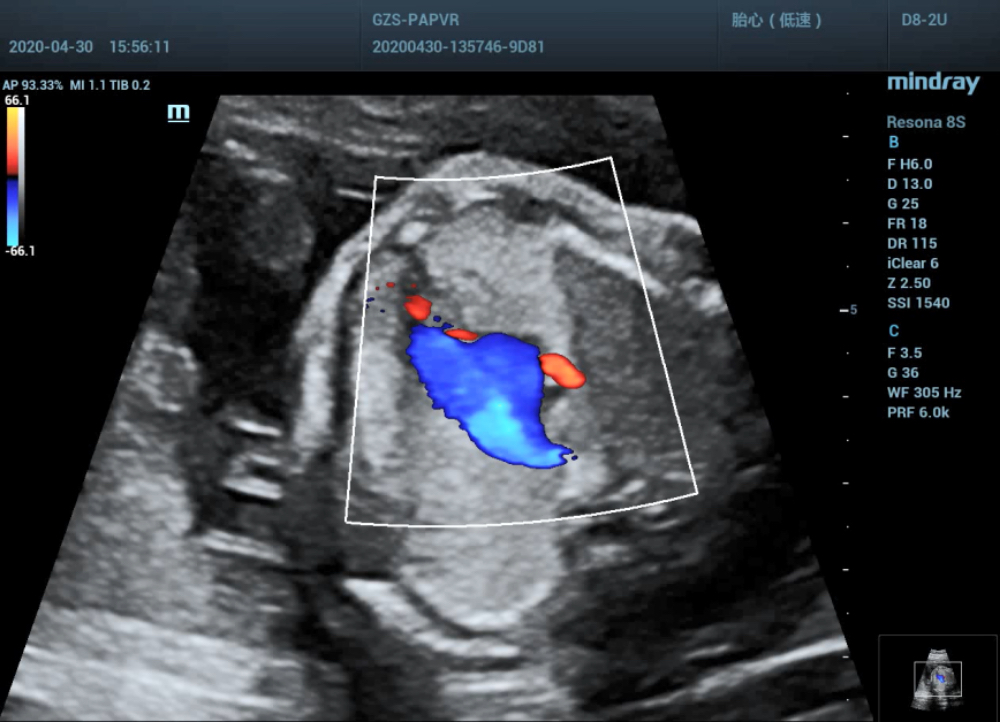
- Low-level four chamber view shows LSPV and LIPV return to the coronary sinus that makes the posterior wall of the coronary sinus protruded and inner diameter broadened.
- Color Doppler shows the blood from LSPV and LIPV flowed through the coronary sinus and directly flowed into the right atrium, which crossed the right superior and right inferior pulmonary veins in a dislocation rather than confluence.
- Four chambers view shows the distance between posterior wall of left atrium and aorta was broadened (posterior-left atrium space index increased).
Misdiagnosis Analysis
- Four chambers view of color doppler seems to show that all pulmonary veins return to the left atrium. Actually, LSPV and LIPV only brush below the LV rather than drain into the left atrium.
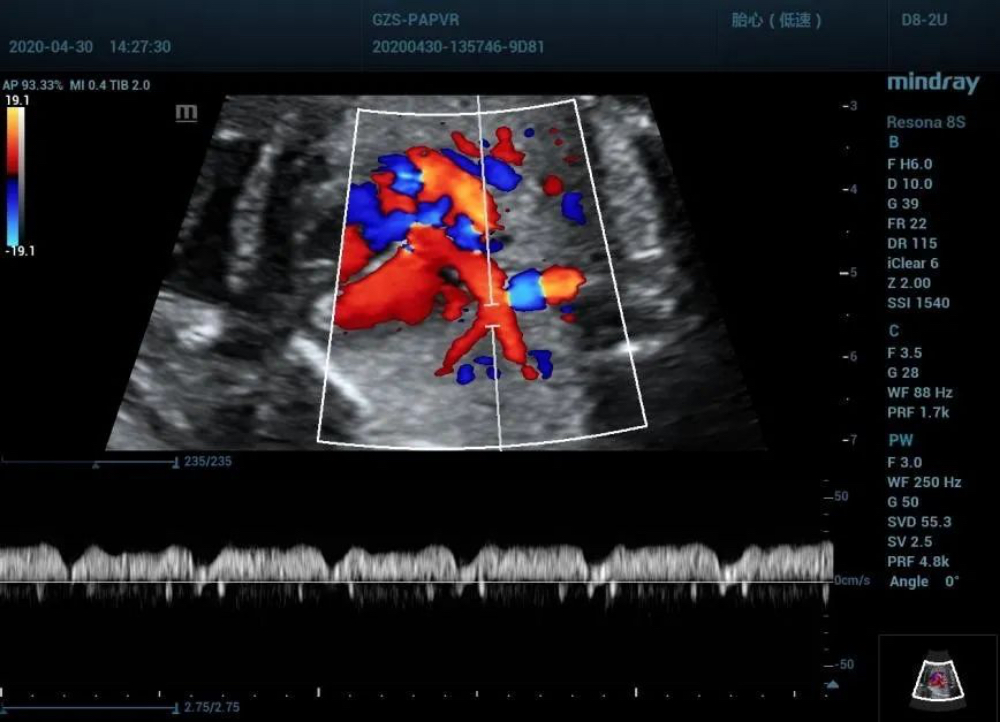
- Normalization of left lower pulmonary vein spectrum.LIPV connected directly with the right atrium by the dilated coronary sinus. While during the cardiac cycle, the pressure changes in the right atrium can be transmitted to the pulmonary vein which prone to jump to conclusions.
Discussions
Partial anomalous pulmonary venous return (PAPVR) is a rare congenital cardiovascular condition in which one or more (but not all) of the pulmonary veins drain into the right atrium or systemic circulation rather than in the left atrium.
- Ectopic drainage pathway
According to the location of ectopic drainage, intracardiac, supracardiac and subcardiac are concluded. Intracardiac type is the most common type while subcardiac type is rare. Right-sided PAPVR is considered one of the most frequent types. And the most common direct drainage of right pulmonary vein is right atrium. Generally, the right pulmonary vein ectopic drainage often leads to the superior vena cava, inferior vena cava, right atrium, azygos vein, portal vein and hepatic vein. On the other hand, anomalous pulmonary venous drainage often leads to the left cephalic brachial vein, coronary sinus and hemiazygos vein.
- Hemodynamics
One or more pulmonary venous blood is drained to the venous system of the systemic circulation, and part of the pulmonary venous blood is drained to the left atrium(LA), resulting in left-to-right shunting, pulmonary hypertension (PH), right heart insufficiency(CHF), and sinus node dysfunction would happen.
- Clinical symptoms
The severity of clinical symptoms depends on the degree of left to right shunt. Patients with small shunt flow may not have any clinical symptoms for life. While patients with multiple anomalous PVD often have chest pain, palpitation and dyspnea, and some patients may have severe PH.
- Treatment and Prognosis
In principle, surgical treatment have to be done for these children. Others believe that when a single anomalous pulmonary venous drainage (APVD) occurs, follow-up observation can be carried out as the small shunt volume and without other malformations. However, patients with more than 2 ectopic drains should be treated with early surgery because of large drainage volume, which is equivalent to large atrial septal defect.
Transposition suture of atrial septum, anastomosis of pulmonary vein and left atrium with ectopic drainage are used for surgical. Intra-atrial patch repair and vertical venous left atrial appendage anastomosis are also often used. Drainage of partial pulmonary venous malformations is effective as early postoperative mortality is less than 4%.
References:
1. Rong Jin, Yi Luo, Pei Cheng, et al. Diagnosis and treatment of partial anomalous pulmonary venous drainage. Chinese Journal of medicine, 2008, 88 (15): 1066-1068
2. Yoshihara K, Ozawa T, Sakuragawa H, et al. 1998. Surgical treatment of total anomalous pulmonary venous connections-clinical aspects of pulmonary venous obstruction. J. Tnorac. Cardiovasc Surg, 46:1126-1132.