Special thanks to Dr. Pedro Forcada MD PhD for sharing this case.
Introduction
Evaluation of carotid arteries and plaques in this region by means of PW and color Doppler has been useful up to date to diagnose carotid disease and its degree of severity and define treatment strategies. However, some limitations due to plaque characteristics like length, tortuosity, heterogeneity, and calcifications that produce complex flow patterns pose serious difficulties to be analyzed by PW and color Doppler, also limited by angle and spatial resolution, and sometimes make difficult or inaccurate the quantification of the stenosis degree and plaque vulnerability.
A new Doppler technology based on Vector Flow Imaging (VFI), a representation of flow supported by high frame rate Doppler using multidirectional blocks technology enables the analysis of complex high-speed flow patterns, represented by omnidirectional Doppler flow vectors with proportional color and size. This new development is called V FLOW.
With a wider Region of Interest (ROI) than PW Doppler and more precise vectorial representation than color grading, using V FLOW it is possible to measure velocity and flow gradients at different sections of a vessel, within the same beat, the wall shear stress in different regions of the vessel wall or plaques and the degree of flow turbulence. This advance conducts to a new era of quantitative and qualitative vascular flow evaluation, going into deep of complex flow patterns and the physiopathology of the vessel wall structure and function. This may lead to a better understanding of the evolution of atherosclerotic lesions from their beginning to their complications.
Two cases of different patients, with different types of plaques in the same vessel and region (LCCA bulb and common artery) are presented to show the application of this new technology.
Clinical Cases
1. Medical history: Two cases, one is O. M. 64 y.o female and the other is S.A. 40 y.o. female, both stage I hypertensives, OM was also dyslipemic treated with rosuvastatin. Both with hereditary traits for hypertension and CV disease. Without antihypertensive therapy but OM received hydrochlorothiazide for prevention of renal lithiasis. Referred for carotid US vascular screening for primary prevention.
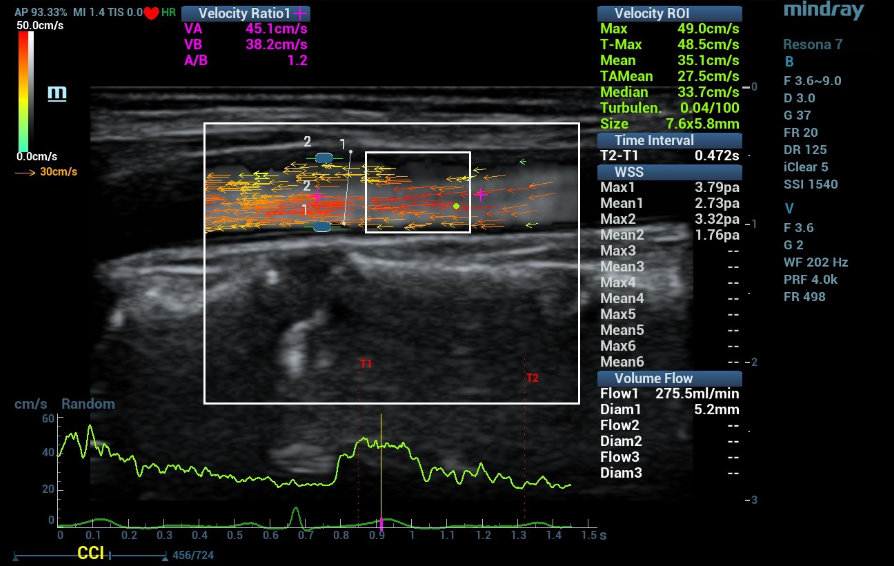
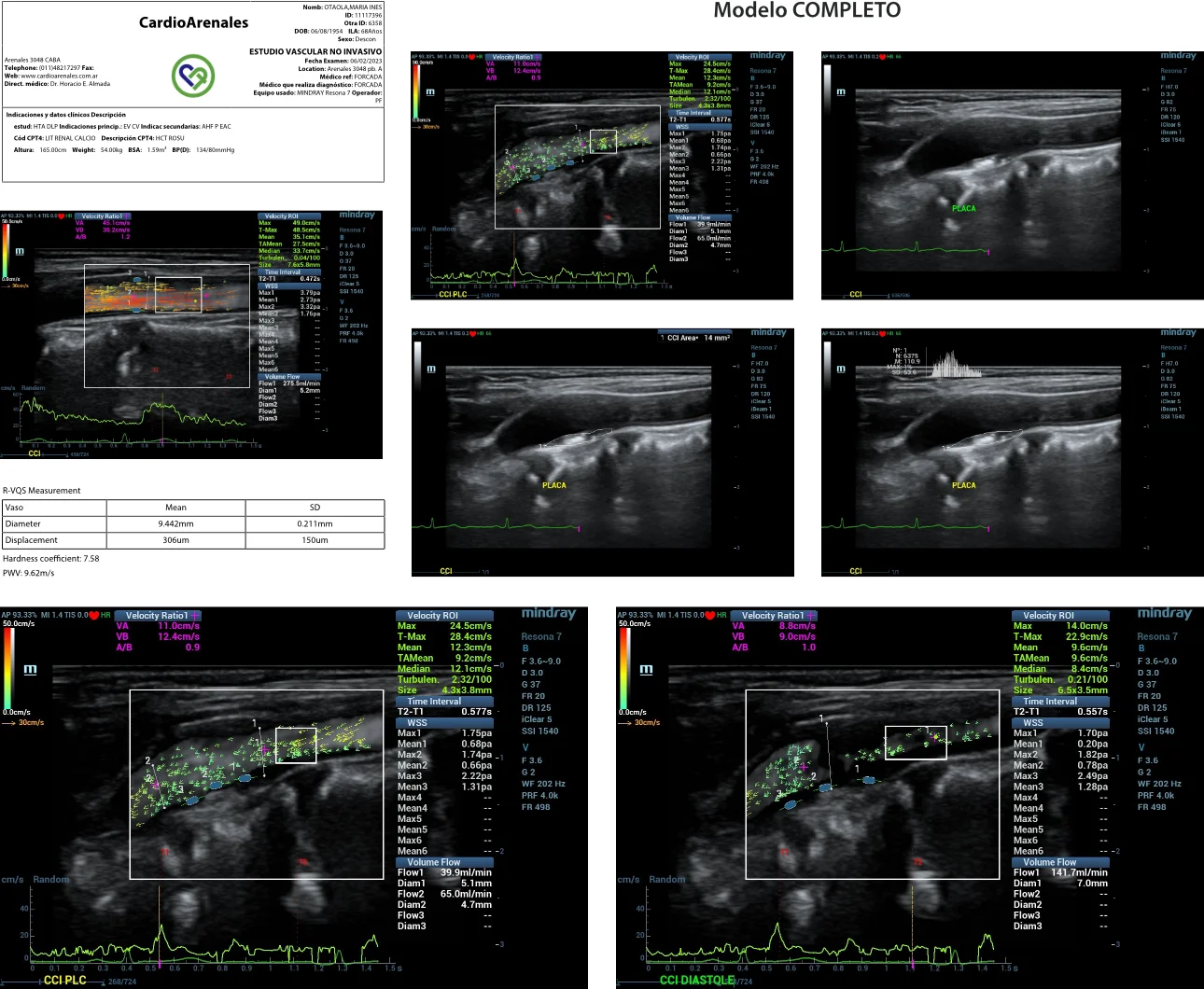
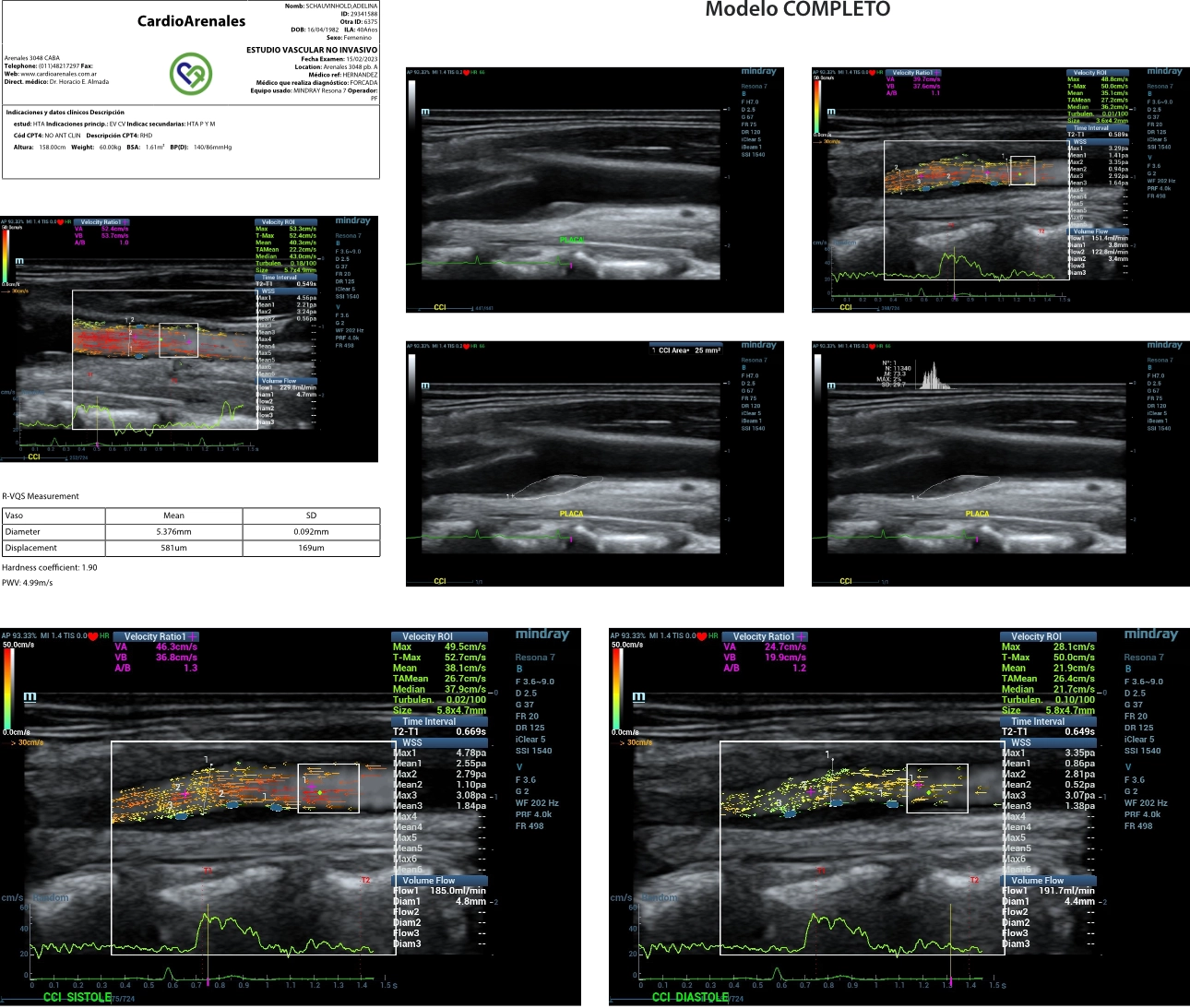
2. US findings: Carotid atherosclerotic plaques in left carotid artery bulb. Evaluations: Complete US investigation of carotid and femoral arteries. Evaluation of Pulse Wave Velocity and endothelial function test using forearm ischemia hyperhemia were performed. Analysis of plaques in left common carotid artery included, plaque area, B Hist plaque composition analysis (Grey Scale Mean GSM), V FLOW parameters speed gradient, flow, WSS and turbulence) and also LCCA were evaluated using V FLOW and RVQS stiffness evaluation (Pulse Wave Velocity (PWV) and Hardness coefficient). (Table 1)

3. Laboratory examination and other radiology image: Normal Echocardiogram and negative exercise test for ischemia in both cases.
4. Diagnosis: Preclinical Atherosclerotic plaques. Increased CV risk reclassified according to US findings. Different structural and hemodynamic patterns of atherosclerotic plaques in the same territory are described.
LCCA speed and flow were comparable, but the stiffness was higher in the LCCA of the Stiff plaque (PWV 9,6 vs. 5 m/s and Hardness coefficient 7,6 vs 1,9) compared to soft plaque LCCA. The Stiff plaque showed a smaller area (14 vs 25 mm2), higher GSM (111 vs 73 GS) and lower values of WSS in the proximal shoulder (0,68 vs 1,41 Pa), the tip (0,66 vs 0,94 Pa) and distal shoulder (1,3 vs. 1,64 Pa) than the soft plaque. The pattern of the WSS shows a “depression” in the proximal shoulder of the stiff plaque and in the top center of the soft plaque, probably linked to the expansion of the last one (almost 10% compared with 0% of the stiff plaque, see bulb diameter syst/diast). (Table 1)
Discussion
Detection of Preclinical Atherosclerosis has been suggested in recent guidelines to reclassify Cardiovascular Risk in patients at low and intermediate risk. Atherosclerotic plaques can modify risk due to the Atherosclerotic Load (surface or volume of plaques), number of vessels involved or its vulnerability.
It has been described that plaques differ between high risk, symptomatic patients (soft plaques or “expanding plaques”) and clinically stable ones (stiffer or hard plaques “non expanding plaques”). The hemodynamic pattern and the structural and functional properties of the surrounding vessel walls can be different in each case and may condition the evolution of the plaques and patient`s clinical evolution. (a soft plaque with turbulent flow with increased or reduced wall shear stress can be considered a “vulnerable” or “at risk” plaque)
Conclusion
Two cases of hypertensive patients are presented with two characteristic plaques in the left carotid artery, one is soft (OM) and the other (SA) is stiff. The hemodynamic behavior using V FLOW (speed gradient, flow, WSS at different points of plaque surface) in each case, were analyzed and compared.
The neighboring artery of the hard plaque was stiffer compared with the soft plaque and the expansion of the first plaque lower. At comparable levels of speed and flow and negligible levels of gradient, the WSS behavior was different in the stiff plaque than in the soft plaque, showing different vulnerable regions in each one. These findings could lead to a better comprehension of the development and evolution of atherosclerotic plaques and eventually follow up the response to treatment (statins or specific CV treatments). (Graphics 1 Stiff Plaque Graphics 2 Soft Plaque)
References:
[1] Mancia G, Kreutz R, Brunstrom M on behalf of The Task Force for the management of arterial Hypertension of the European Society of Hypertension: 2023 ESH Guidelines for the management of arterial hypertension Journal of Hypertension 2023, 41:000–000. DOI:10.1097/HJH.0000000000003480.
[2] Paini A, Boutouyrie P, Calvet D et al: Multiaxial Mechanical Characteristics of Carotid Plaque: Analysis by Multiarray Echotracking System. Stroke 2007;38;117-123.
[3] Chatzizisis Y, Ahmet Umit Coskun A, Michael Jonas M, et al: Role of Endothelial Shear Stress in the Natural History of Coronary Atherosclerosis and Vascular Remodeling. J Am Coll Cardiol 2007;49:2379–2393.
[4] Arbab-Zadeh A, Fuster V: The Myth of the “Vulnerable Plaque” Transitioning From a Focus on Individual Lesions to Atherosclerotic Disease Burden for Coronary Artery Disease Risk Assessment. J Am Coll Cardiol 2015;65:846–855.
[5] Forcada P: Twenty Years of Non-Invasive Vascular Evaluation: from Bench to Bedside from Theoretical to Precision Medicine. J Non Invasive Vasc Invest 2022, 7: 030 DOI: 10.24966/NIVI-7400/100030.
[6] Forcada P: Study of Arterial Function and Remodelling by Using Radiofrequency and a New Multidirectional Doppler Technology. J Angiol Vasc Surg 2021, 6: 056. DOI: 10.24966/AVS-7397/100056.
[7] Forcada P, Che Cheung K: Comparison of Regional Vs Local Arterial Parameters Using New Us Technology. J Clin Epid Toxic, 2021; 2(1): 1-2.
[8] Yinghui Dong, Shaofu Hong, Di Song, et al: Blood Flow Turbulence Quantification
of Carotid Artery with a High-Frame Rate Vector Flow Imaging. J Ultrasound Med 2022; 9999:1–10.
[9] Yi-Jie Qiu, Juan Cheng, Qi Zhang et al: Clinical Application of High-Frame-Rate Vector Flow Imaging in Evaluation of Carotid Atherosclerotic Stenosis. Diagnostics 2023, 13, 519. https://doi.org/10.3390/diagnostics13030519.