Tackling Clinical Hurdles: Mindray's Innovative Approach
Clinical Hurdles
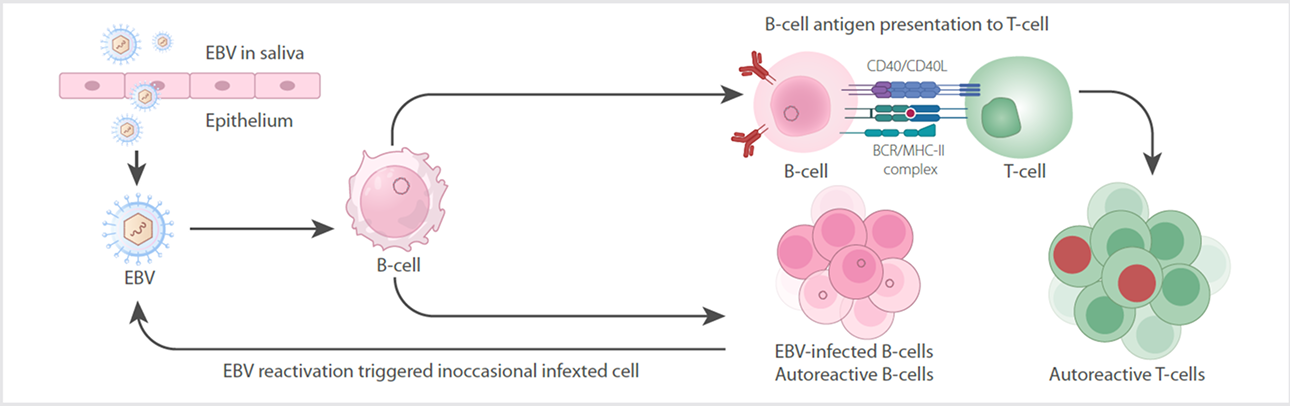
Diagnosing infectious mononucleosis (IM) , primarily caused by Epstein-Barr virus (EBV), faces several clinical challenges due to itsnonspecific symptoms, overlapping presentations with other conditions, and limitations in current diagnostic methods [1,2]. Keychallenges include:
1. Nonspecific Symptoms:
IM often presents with fever, fatigue, pharyngitis, and lymphadenopathy—symptoms common to other viral infections (e.g.,streptococcal pharyngitis, cytomegalovirus). This overlap complicates differential diagnosis without targeted testing.
2. Limitations of Traditional Tests
Heterophile Antibody Tests (e.g., Monospot): False negatives early in infection (sensitivity ~70–90%) and in young children/immunocompromised patients. False positives from cross-reactivity with other conditions (e.g., lupus, rubella).
EBV-Specific Serology (e.g., IgM/IgG): More accurate but costly and time-consuming, limiting use in routine settings.
3. Atypical Presentations
Atypical Lymphocytes : While hallmark IM findings, they also occur in other infections (e.g., toxoplasmosis, HIV) and malignancies,requiring careful interpretation.
Hematologic Overlap : IM may mimic hematologic disorders (e.g., leukemia) due to reactive lymphocytosis, necessitating additionaltests like flow cytometry.
Mindray's Innovative Solution
Mindray realized accurate screening of IM patients through utilizing 3D scatter plot characteristics in the DIFF channel, which meansIM could be flagged in a simple CBC+DIFF (CD) test. Compared to conventional consensus indicators, this alarm demonstrates superiorsensitivity (over 80%) in screening IM cases.
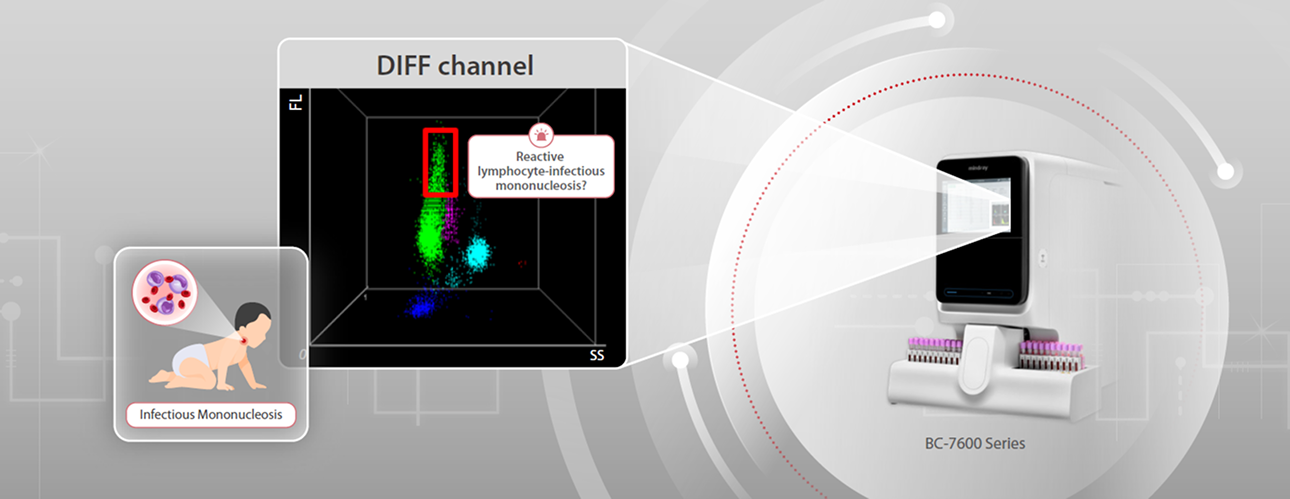
Compared to atypical lymphocyte alarms or high fluorescent cell (HFC) alerts, this alarm exhibits higher specificity (over 96%) for IMdetection. Together, the CD mode shows a great screening efficacy for acute-phase IM patients. After the CD mode flags “ReactiveLymphocyte-Infectious mononucleosis?”, the reflex rule would be triggered to prepare blood smear for morphological analysis,assisting doctors to screen IM precisely and efficiently.
Unveiling the Real Culprit Behind a Young Boy's Fever
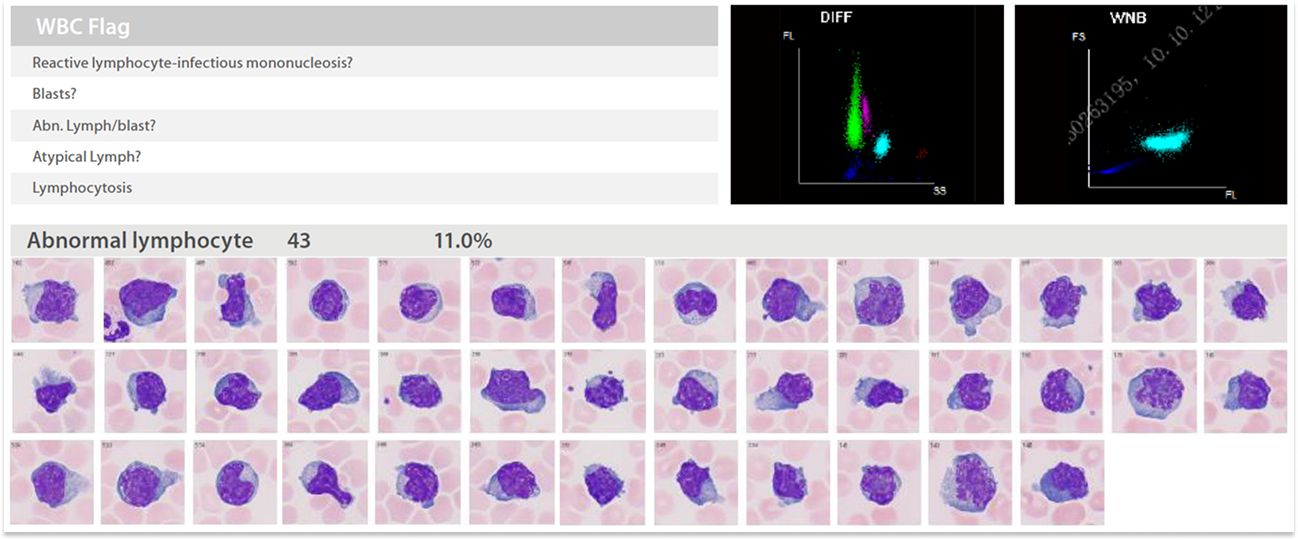
On 28th June, 2024, a 7-year-old boy presented to the outpatient clinic with: cough for 5 days, fever (peak temperature 37.9°C) for 3days. The peripheral blood sample was sent to the lab for analysis. Abnormal scatter plot from Mindray BC-7900, triggered anautomated alarm: "Reactive Lymphocytes-Infectious Mononucleosis?" After that, peripheral blood smear was prepared for review andit was reported that the percentage of reactive lymphocytes was 11% .
On 29th June, the boy was admitted. Physical examination revealed bilateral cervical lymphadenopathy (multiple bean-sized nodes,soft, well-defined, non-tender), mild periorbital edema, tonsillar enlargement (Grade II) with exudate. Combined with blood smearresults, Infectious mononucleosis (IM) was suspected. In the afternoon, the EBV Capsid Antigen (VCA) IgM Antibody test result wasreported, 173.00 U/mL (positive), confirming acute-phase EBV infection . Eventually, combined all the laboratory results, the boy wasdiagnosed with IM, bronchitis , and mycoplasma Infection.
Following accurate diagnosis, appropriate treatment was prescribed and consequently the boy was discharged in stable condition.
Conclusion
Reviewing the case, the BC-7900's initial alarm (”Reactive Lymphocyte - Infectious Mononucleosis?”) served as a critical diagnosticclue, steering subsequent investigations toward confirmatory testing. Especially in pediatrics or children's hospitals, this technologycan assist physicians in distinguishing children infected with EBV from those with other virally-induced similar symptoms. Thisultimately ensures patients receive correct diagnosis and treatment.
References:
[1]Bu, G.-L., Xie, C., Kang, Y.-F., Zeng, M.-S., & Sun, C. How EBV Infects: The Tropism and Underlying Molecular Mechanism for ViralInfection. Viruses, 14(11), 2372 (2022).
[2]Shi T, Huang L, Luo L, Yu Q, Tian J. Diagnostic value of serological and molecular biological tests for Infectious mononucleosis byEBV in different age stages and course of disease. J Med Virol 93, 3824–3834 (2021).
[3] Martin, E., Winter, S., Garcin, C. et al. Role of IL-27 in Epstein–Barr virus infection revealed by IL-27RA deficiency. Nature 628,620–629 (2024).
[4]Dunmire, S. K., Hogquist, K. A. & Balfour, H. H. Infectious mononucleosis. Curr. Top. Microbiol. Immunol. 390, 211–240 (2015).
[5]Rasheed A and Khan G (2024) Epstein-Barr virus, vitamin D and the immune response: connections with consequences for multiplesclerosis. Front. Immunol. 15:1503808. doi: 10.3389/fimmu.2024.1503808
