

Hemabook Chapter 19: Have You Noticed Neutrophil Inclusions in the Thrombocytopenia Smear?
2022-11-10

About Thrombocytopenia
Thrombocytopenia is the disorder of platelet count decreased possibly caused by a variety of pathophysiological mechanisms, including pseudothrombocytopenia, hemodilution, decreased platelet generation, increased platelet consumption, increased platelet sequestration, and increased platelet destruction.

Perioperative thrombocytopenia is commonly observed in clinical patients. The broad definition and grading criteria of thrombocytopenia have a limited role in clinical practice. Hematological consultation should be considered to instruct the diagnosis and treatment of patients with non-emergency surgery or postoperative thrombocytopenia [1]. Comprehensive analysis of the invasive test results and the differentiation of etiology (or pathophysiological mechanism) for patients with thrombocytopenia are essential for thrombocytopenia treatment, which is a challenge for all clinical departments and laboratories.
What are the findings during thrombocytopenia sample analysis? Do you ever notice the neutrophil inclusions in the thrombocytopenia smears? Here is a case reported by Dr. Cai Qi from Ruijin Hospital, Shanghai Jiaotong University School of Medicine, one of the top national comprehensive hospitals in China.
A Thrombocytopenia Case from Ruijin Hospital
The patient is a 45-year-old male diagnosed with thrombocytopenia for more than two years. In early 2022, the patient was observed signs of hyperparathyroidism in a physical examination and the ultra-sound radiography showed multiple hypoechoic lesions in the left parathyroid gland.
Further investigations were performed and the patient was diagnosed with a left thyroid nodule (C-TIRADS 3). The biopsy result indicated papillary carcinoma and surgical resection was required. Due to the previous history of thrombocytopenia, the patient visited the hematology outpatient clinic of Ruijin Hospital for advice on surgical contraindications. The medical record showed that the last platelet (PLT) count (another hospital, Dec. 2021) was 14 × 109/L.
On Feb. 21, 2022, the patient's hematology was analyzed by Mindray Auto Hematology Analyzer BC-6800Plus in Ruijin Hospital.
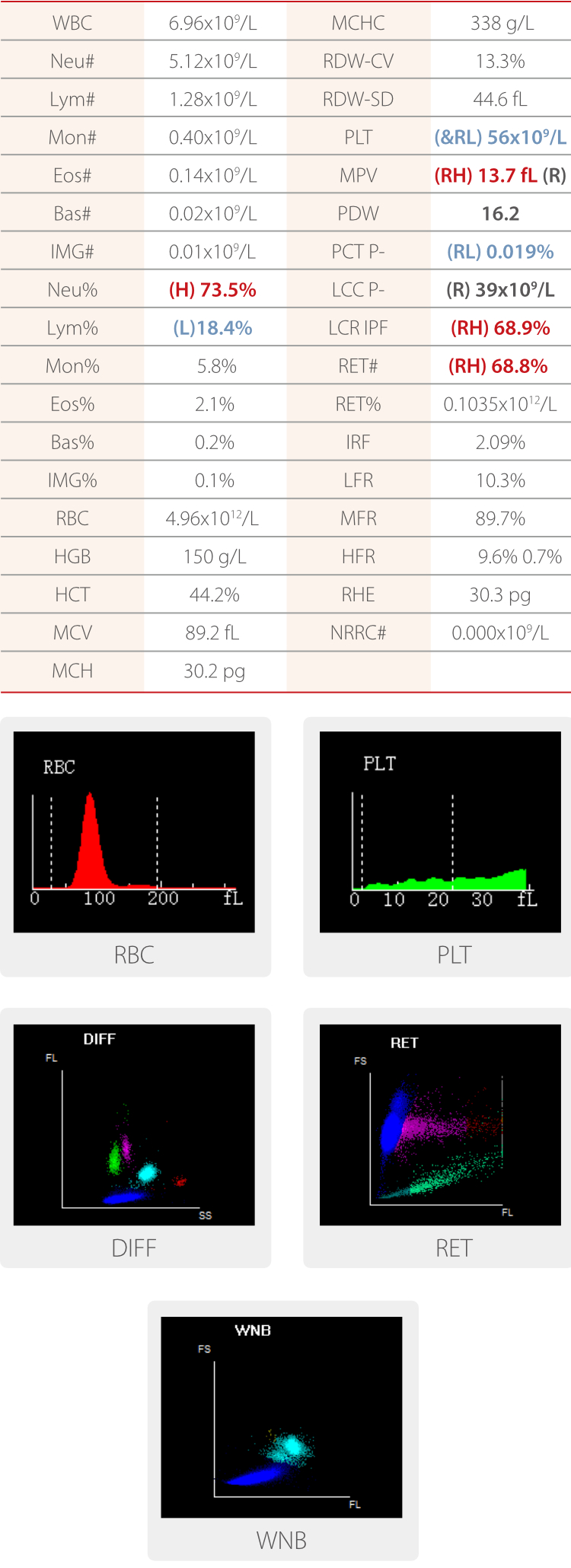
Platelet count decreased was indicated by test items marked with &RL flags (&: corrected; R: to be re-examed; L: low). The PLT count tested by Mindray BC-6800plus was 56 × 109/L, higher than the patient's previous platelet test results. Therefore, RUO (research use only) parameters were investigated for more detail.

More details were provided, including PLT-I 14 × 109/L and PLT-O 56 × 109/L. The PLT histogram showed an elevated tail and the PLT-O scattergram showed highlighted clusters in the larger PLT regions, indicating the presence of large platelets.
The blood smear was automatically prepared by Mindray Slide Maker & Stainer SC-120 and analyzed in the "WBC + RBC + PLT" mode by Mindray Automatic Digital Cell Morphology Analyzer MC-80.
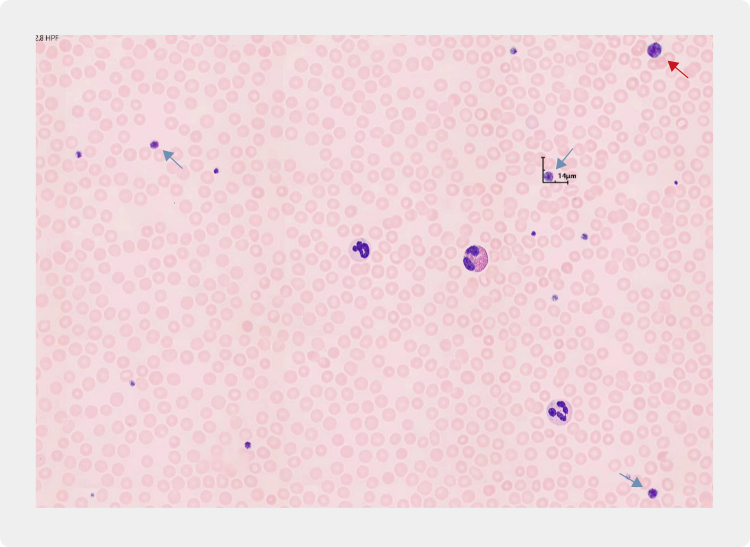
In the RBC & PLT image, many large platelets were presented. The total platelet count measured by MC-80 was 63 × 109/L. The WBC images were also investigated and it was worth noticing that a large number of Döhle bodies were observed in the neutrophils.

The abnormal neutrophil inclusions (Döhle bodies) found in this patient, as well as the presence of large platelets and thrombocytopenia, allowed laboratory doctors to quickly associate with the peripheral blood morphology of MYH9 mutation-related disease (MYH9-RD). The report was sent to the clinical department and investigations were arranged to confirm the finding.
Later on, the patient was admitted to the hospital on Mar. 6, 2022, completed relevant preoperative examinations and preparations, and underwent subtotal unilateral thyroid gland removal (left thyroidectomy) under general anesthesia on Mar. 7, 2022. The operation was successful and the patient recovered well. There was no bleeding from the incision and the patient was discharged from the hospital on Mar. 9, 2022.

Thrombocytopenia and Conclusion
MYH9 is a large gene spanning more than 106 kb pairs on chromosome 22q12.3-q13.2. It is composed of 40 exons and encodes non-muscle myosin heavy chain IIA (NMMHC IIA), a protein with a relative molecular mass of about 224,000 and essential for the non-muscle cytoskeleton with its wide expression in tissues or cells such as platelets, granulocytes, renal cells, cochlear cells, and lens cells [2].
MYH9-RD is one of the most common types of hereditary thrombocytopenia, with an incidence of about 1/100,000. It is mainly featured with peripheral blood thrombocytopenia, accompanied by large platelets and different degrees of bleeding tendency and infection, as well as progressive renal failure, hearing loss, or cataracts. Four overlapping syndromes, known as May-Hegglin anomaly, Epstein syndrome, Fechtner syndrome, and Sebastian platelet syndrome, describe different clinical manifestations of MYH9-RD. MYH9-RD is autosomal dominant and characterized by large Döhle bodies in granulocytes, especially neutrophils, accompanied by large platelets and thrombocytopenia [3].
Most MYH9-RD-related thrombocytopenia is not serious and the disease is distinguishable by the findings in peripheral blood smears, i.e., the characteristic morphological features of thrombocytopenia with large platelets and large Döhle bodies in massive neutrophils. The relationship between MYH9 genotype and clinical phenotype has been confirmed. Clinical studies have shown that thrombopoietin mimetics are possibly effective in thrombocytopenia treatment and bleeding tendency control in relevant patients [4].
Case analysis of MYH9-RD-related thrombocytopenia
For MYH9-RD patients, laboratory examinations are particularly important. Due to a large number of large platelets, the electrical impedance method may not be incompetent for counting platelets correctly. This may lead to a false report of a low PLT count. Such a situation must be detected and dealt with in time. Although the current new hematology systems and detection methods can avoid the occurrence of such errors to a great extent, the accuracy of the results must be preliminarily evaluated by laboratory physicians with the PLT histogram and determined based on the blood smear microscopic examination. The results should be reviewed for confirmation before being reported to the clinical physicians to avoid the incorrect assessment of patient conditions on thrombocytopenia.
Morphological examination of the peripheral blood cells is also critical in assisting MYH9-RD diagnosis. The morphological examination for peripheral blood smears of patients with thrombocytopenia should include the morphology of RBC and WBC, as well as the detection of fragmented RBCs and morphological abnormalities of WBCs. In this case report, the observation of neutrophil inclusions is essential for the rapid diagnosis of MYH9-RD.
Mindray MC-80 identifies peripheral blood leukocytes accurately and provides automatic pre-classification and platelet estimation, which is superior to the time-consuming and labor-intensive traditional manual platelet counting of peripheral blood smears. MC-80 also automatically identifies all the RBCs and platelets within the set scanning range and conducts cell counting. The combination of the RBC count measured by the hematology analyzer and the total platelet count measured by MC-80 significantly facilitates the work of the laboratory physicians while improving the accuracy of the reported results.
Acknowledgement
We thank you Dr. Cai Qi (Ruijin Hospital, Shanghai Jiaotong University School of Medicine, P.R. China) for providing the informative clinical case.
References
[1] A. Nagrebetsky, H. Al-Samkari, N. M. Davis, D. J. Kuter, J. P. Wiener-Kronish. Perioperative thrombocytopenia: evidence, evaluation, and emerging therapies. British Journal of Anaesthesia, 122 (1): 19e31 (2019)
[2] Balduini CL, Pecci A, Savoia A. Recent advances in the understanding and management of MYH9-related inherited thrombocytopenias. Br J Haematol. 2011 Jul; 154 (2): 161-74.
[3] Althaus K, Greinacher A. MYH9-related platelet disorders. Semin Thromb Hemost. 2009 Mar; 35(2): 189-203.
[4] Barros Pinto MP, Marques G. MYH9 Disorders (May-Hegglin Anomaly) the Role of the Blood Smear. J Pediatr Hematol Oncol. 2019 Apr; 41(3): 228.


