Ultrasound Journal 40 - Carotid Plaque: Conventional and Innovation Technique
Academic Clinical Specialist APAC Region Johanna Wong

Introduction
Carotid atherosclerotic stenosis is the main cause of ischemic stroke, which can result in long-term disability and increased mortality among the aging population. It has been reported that moderate to severe carotid stenosis (50–99%) affects approximately 9% of individuals over 60 years of age and contributes to 10% of all strokes. The imaging evaluation and ongoing monitoring of symptomatic carotid stenosis are critically important for the prognosis and quality of life of elderly patients.
Conventional Ultrasound is the first-line medical imaging modality for the assessment of the hemodynamics of carotid stenosis. The common ultrasound manifestations of carotid atherosclerotic stenosis are the increase in carotid intima media thickness, atherosclerotic plaque formation, local lumen stenosis, and increased peak systolic velocity at the stenosis site.
Recent advancements, such as vector flow ultrasound, emphasize the assessment of a new ultrasound parameter, ''wall shear stress'' (WSS), which may serve as a potential hemodynamic factor influencing plaque instability. By calculating WSS and evaluating related wall deformation, we can glean insights into the plaque composition and its likelihood of rupture, thereby enabling the assessment of future cerebrovascular event risks for individuals affected by carotid atheroma.
Clinical case
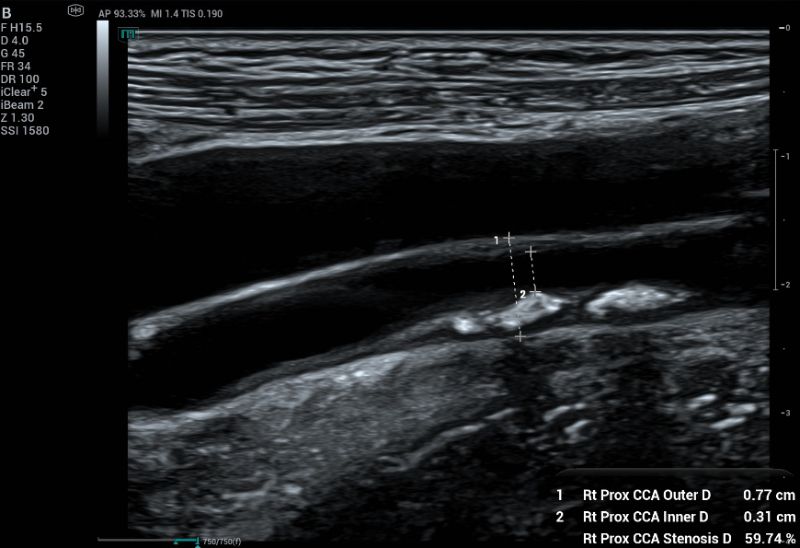
A 50-year-old female came for health screening with no symptoms. Carotid ultrasound assessment was done bilaterally. A plaque measuring 2.36 x 0.34 cm (Figure 1) was found on the right distal CCA.
Color Doppler is a standard tool to assess stenosis and overall flow. CF shown reversal flow at the stenosed area (Fig 2).

To measure percentage of stenosis, diameter-based measurement (Fig 3) remains the most widely accepted method to quantify carotid stenosis. However, for plaques that are non-circular or crescent-shaped in cross-section, a single diameter measurement can significantly underestimate the true severity of the narrowing.
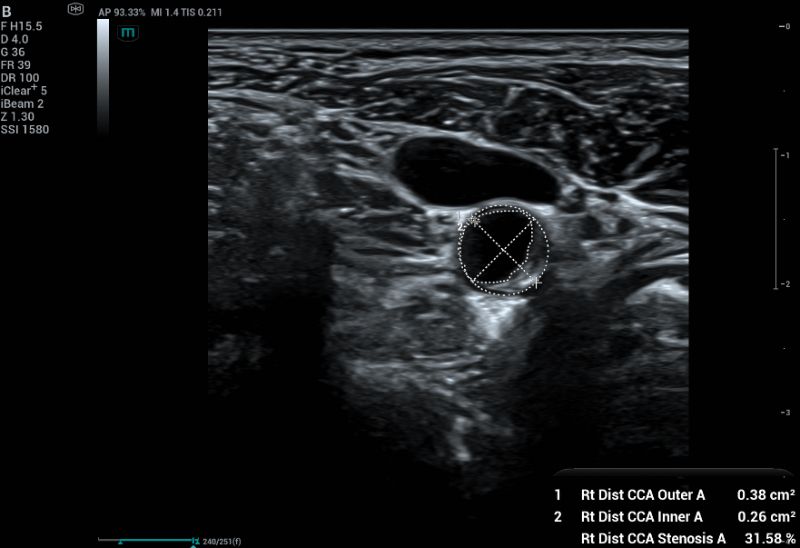
Area-based measurement using cross-sectional imaging (Fig 4), the area of the residual lumen can be directly measured. This method can more accurately quantify stenosis in plaques that are irregularly shaped and asymmetric in cross-sectional images. However, the non-linear relationship between diameter and area (A=πr2) means that the area method can yield higher percentages of stenosis than the diameter method.
Relying on a single view can lead to inaccuracies. Using both longitudinal and axial views provides a more complete picture of the plaque and the vessel, ensuring a more accurate measurement of stenosis.
The combination of visual assessment and Doppler velocity analysis is the standard for a complete carotid ultrasound study.
Advance Imaging Technique
Mindray premium ultrasound system Resona A20 provides a comprehensive vascular solution.
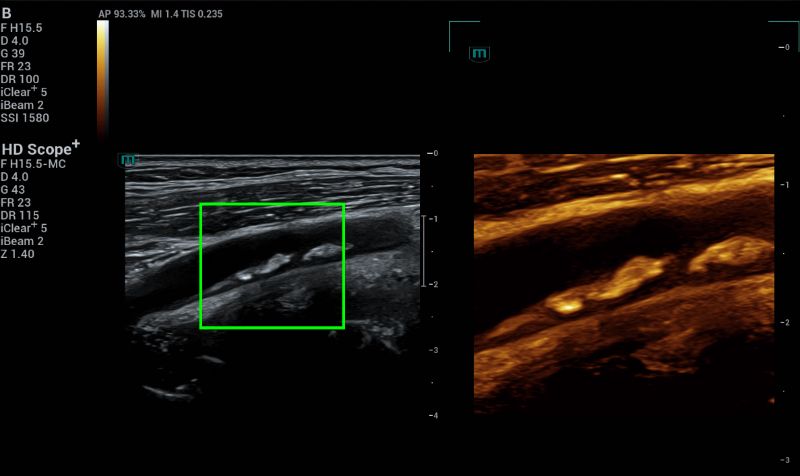
HD Scope+ improves spatial and contrast resolution, allowing for clearer differentiation of tissue types (Fig 5). This can reveal the complex nature of a plaque, including echogenicity, heterogeneous elements, and lucent cores, which are important for determining its stability and risk.
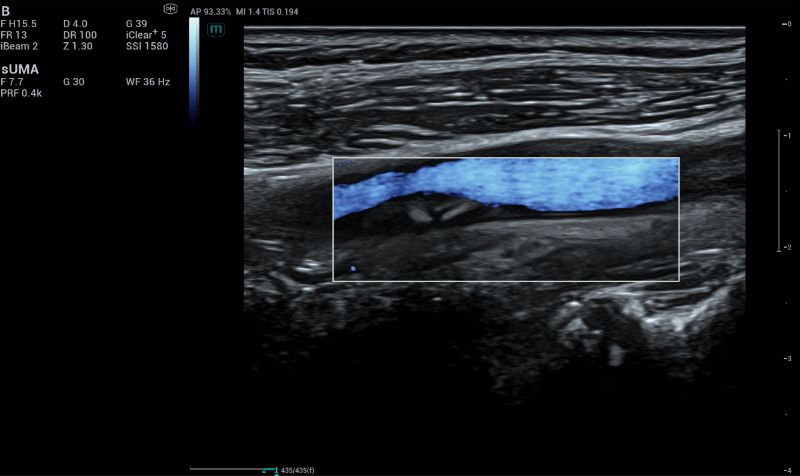
Ultra Micro Angiography (UMA) can reveal subtle, slow blood flow within the plaque itself, which indicates intraplaque neovascularization (IPN) and plaque instability (Fig 6). IPN is a characteristic feature of carotid plaque vulnerability. Lesions with IPN are prone to intraplaque hemorrhage, which is associated with rupture, formation of local thrombi, and distal embolization.
A novel ultrasound-based technology called V Flow demonstrated the dynamic of the blood flow. The fluidity will be displayed with arrows indicating the flow process. Both the magnitude and direction of the flow can be measured at any location in the vessel. V Flow-detected hemodynamic parameters were related to plaque components and plaque vulnerability. V Flow has the potential to be an effective tool for investigating patients with severe carotid plaque.
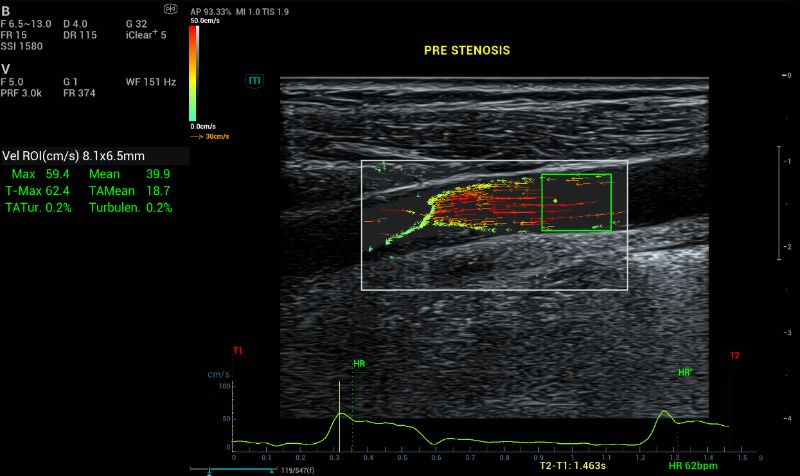
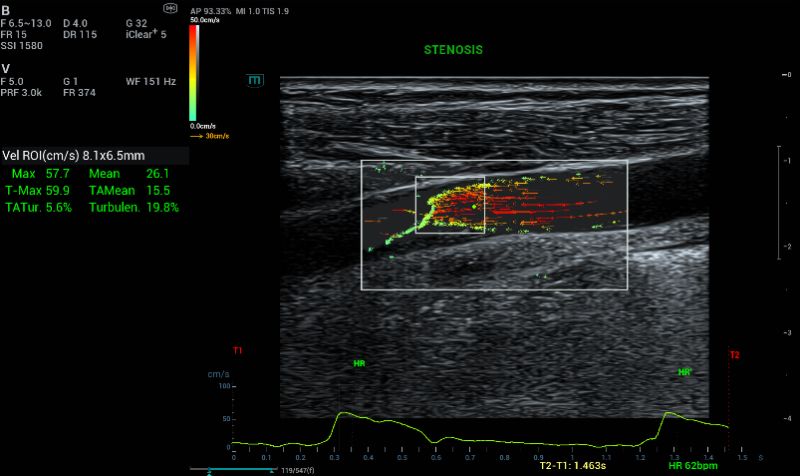
The V Flow dynamic imaging shows that the length of the vector arrows at site of the carotid stenosis was longer than the surrounding vessel wall. The color of vector arrows at the carotid stenosis site was orange or red with faster flow velocity. However, the most common vector arrows at the distal and proximal sites of the stenosis were slower green or yellow vector arrow (Fig 7).
Unlike B-mode and color Doppler US, V Flow is independent of the ultrasound angle; therefore, V Flow uses a high frame rate to track high speeds in real time and to intercept transient flow phenomena resulting in a high space–time resolution.
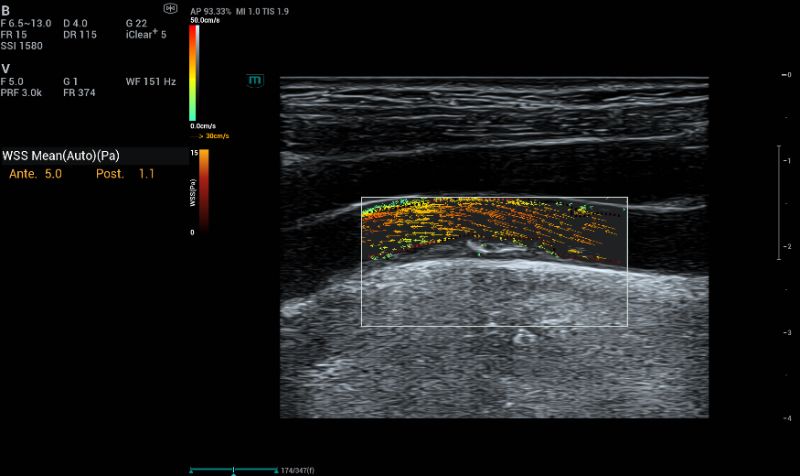
V Flow can quantify a new ultrasound parameter defined as “wall shear stress” (WSS), representing the friction force exerted by the blood flow on each point of the endothelial atheroma surface. Considering that a plaque is strongly affected by hemodynamic changes due to shear stress, WSS could became a determining factor in assessing plaque evolution and stratifying patient risk, even for asymptomatic patients.
Low WSS (<0.4 Pa) may influence the morphology and function of endothelial cells, closely associated with intimal thickening and the formation of atherosclerosis. High WSS values (>7Pa) for an atherosclerotic surface are potentially indicative of plaque vulnerability and so could be predictive of future complications related to thromboembolic events. At the upstream sides of carotid stenosis, plaque with a lower mean WSS was associated with decreased fibrous tissue. At the peak of carotid stenosis, meanWSS was higher in the plaques with intraplaque hemorrhage and intraplaque neovascularization. High WSS is generally linked to plaque rupture, while low WSS facilitates plaque development.
Turbulence Index (Tur) is higher in vulnerable plaque, showed more intraplaque hemorrhage, thrombus, and thinner fibrous cap thickness. When the Tur value is equal to or close to 0, the flow is laminar or approximately laminar.
Conclusion
Based on the vascular multiparameter study, the right CCA plaque in this patient showed relatively stable.
Clinical results indicate that the new method yields significantly more detailed insights into the various flow patterns within the carotid artery, in comparison to traditional CFM.
This innovative approach, characterized by multiple quantitative parameters, enhances our understanding of blood flow dynamics, which is essential for the diagnosis and treatment of carotid artery conditions.
References:
[1]. Yi-Jie Qiu et al. Clinical Application of High-Frame-Rate Vector Flow Imaging in Evaluation of Carotid Atherosclerotic Stenosis. Diagnostics 2023, 13(3), 519
[2].Emanuele David et al. Imaging of Carotid Stenosis: Where Are We Standing? Comparison of Multiparametric Ultrasound, CT Angiography, and MRI Angiography, with Recent Developments. Diagnostics 2024, 14(16), 1708
[3]. Liuping Cui et al. Carotid Intraplaque Neovascularization and Future Vascular Events in Patients With Asymptomatic Carotid Stenosis. Frontiers in Pharmacology 2022, 13:804810
[4]. Yigang Du. V Flow, A novel visualization of blood flow. Mindray White Paper
[5]. Yachao Zhang et al. Blood Flow Turbulence Measured by High-frame-rate Vector Flow Imaging Conduced to Investigating Advanced Carotid Plaque Vulnerability. Ultrasound in Medicine & Biology 2025, 51(10), 1682
[6]. Yigang Du et al. Wall Shear Stress Measurements Based on Ultrasound Vector Flow Imaging Theoretical Studies and Clinical Examples. J Ultrasound Med 2020; 39:1649–1664
[7]. Yinghui Dong et al. Evaluation of Turbulence Index and Flow Pattern for Atherosclerotic Carotid Stenosis: A High-Frame-Rate Vector Flow Imaging Study. Ultrasound in Medicine & Biology 50 (2024) 549−556