
Thyroid disorders are one of the most common disorders affecting women of reproductive age.
Comprehensive treatment and management can help reduce the risks associated with thyroid disorders. Now, let’s delve into the various types of thyroid disorders and how to manage them during pregnancy[1].
The physiological changes in thyroid function during pregnancy are presented in the following figure.

In the first half of pregnancy, normal levels of maternal thyroid hormone are the guarantee for the normal development of the fetal nervous system. In addition to the mother's thyroid hormone levels, fetal thyroid function is also affected by other factors such as autoantibodies, iodine or I131 and antithyroid drugs.

Due to the unique physiological changes of hormone and the possible clinical influences, it is necessary to establish a normal range for the gestation period and a local reference range to facilitate the clinical evaluation of thyroid hormones.



There are different types of thyroid disorders during pregnancy and the resulting changes in hormone levels are complex[3].

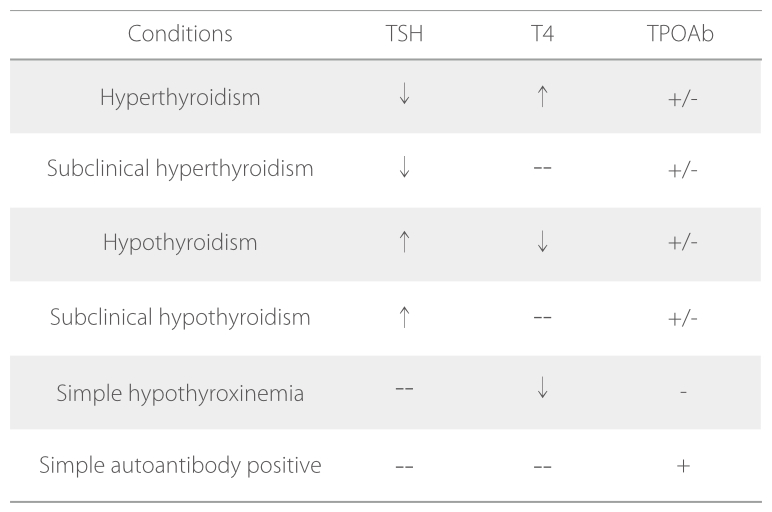
Different types of thyroid disorders may lead to the following clinical conditions on the mother and the baby.

Therefore, many guidelines recommend that thyroid function evaluation be conducted in the early pregnancy of risky population to reduce their risk of developing thyroid disorders throughout pregnancy[13].


Extensive research data has demonstrated that pregnant women are one of the most affected populations by thyroid disorders. Maternal thyroid dysfunction has been associated with a variety of adverse pregnancy outcomes. One of the most effective ways to prevent such adverse outcomes is to evaluate thyroid function in early pregnancy.
Mindray’s chemiluminescence immunoassay products offer thyroid function evaluation solutions with a comprehensive thyroid panel and a complete set of analyzers. In addition, a gestational-specific reference interval has been established for greater ease of application.

References
[1] Peter N. Taylor.Global epidemiology of hyperthyroidism and hypothyroidism. Nature reviews endocrinology. Volume 14 , May 2018, p 301-316.
[2] 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum
[3] 2012, Chinese Journal of Endocrinology and Metabolism, Guidelines for the diagnosis and treatment of thyroid disease in pregnancy and postpartum , Volume 28, Issue 5
[4] Millar LK. Obstet Gynecol,1994, 84:946 –949.
[5] Momotani N. J Clin Endocrinol Metab, 1997,82:3633-3636.
[6] European Journal of Endocrinology (2011) 164 871–876
[7] Krassas GE, Poppe K, Glinoer D. Endocr Rev. 2010
[8] Stephen H. Thyroid 2005, 15(1):60-71.
[9] J Matern Fetal Neonatal Med, Early Online: 1–6 [10] JCEM. 2010 95:4227-4234
[11] Clinical Endocrinology (2011) 74, 513–519 [12] BMJ 2011;342:d2616
[13] 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease during Pregnancy and the Postpartum




