Ultrasound Journal 15 - Carotid Glomus, presentation of a case with diagnosis by multiparametric ultrasound and multimodal imaging
By Ricardo Daniel Alpízar Cruz, Verónica Espinosa Cruz, Alejandro García Peña 2023-07-01

Introduction
Paragangliomas, or also called carotid glomus (GC), belong to a heterogeneous group of neuroendocrine neoplasms dependent on the autonomic nervous system.They are classified, mainly by their function, into secretory (typical of the sympathetic nervous system) and non-secretory (originating from the autonomic nervous system). They develop embryologically from paraganglionic cells of the neutral crest. The most frequent anatomic localization sites are in the intra-abdominal, thoracic and head and neck regions, together representing more than 90% of these neoplasms. Of the head and neck glomus, paragangliomas or glomus of the intercarotid space are the most common. Carotid glomus is more common in women in an age range between 40 and 70 years and presents as a pulsatile tumor, rarely palpable, which causes mass effect on adjacent structures causing as main symptoms dysphagia,syncope or Horner's syndrome.
Evaluation by imaging is essential in paraganglioma for diagnostic suspicion, being the multimodal approach preferred for the provision of information for both diagnosis and surgical planning. The definitive diagnosis is made through histopathology and immunohistochemistry.
This paper presents the case of a 52-year-old patient diagnosed with left carotid glomus.
Clinical case
This is a 52-year-old female patient with a history of ankylosing spondylitis, posterior communicating cerebral aneurysm, resolved by clipping. The patient presented clinically with left otalgia, tinnitus, hemineck pain intensity 8/10 with dorsal irradiation and tachycardia. Metanephrines were requested in urine and serum with negative result, however positive with serotonin and chromogranin , so it was decided a resection surgery.
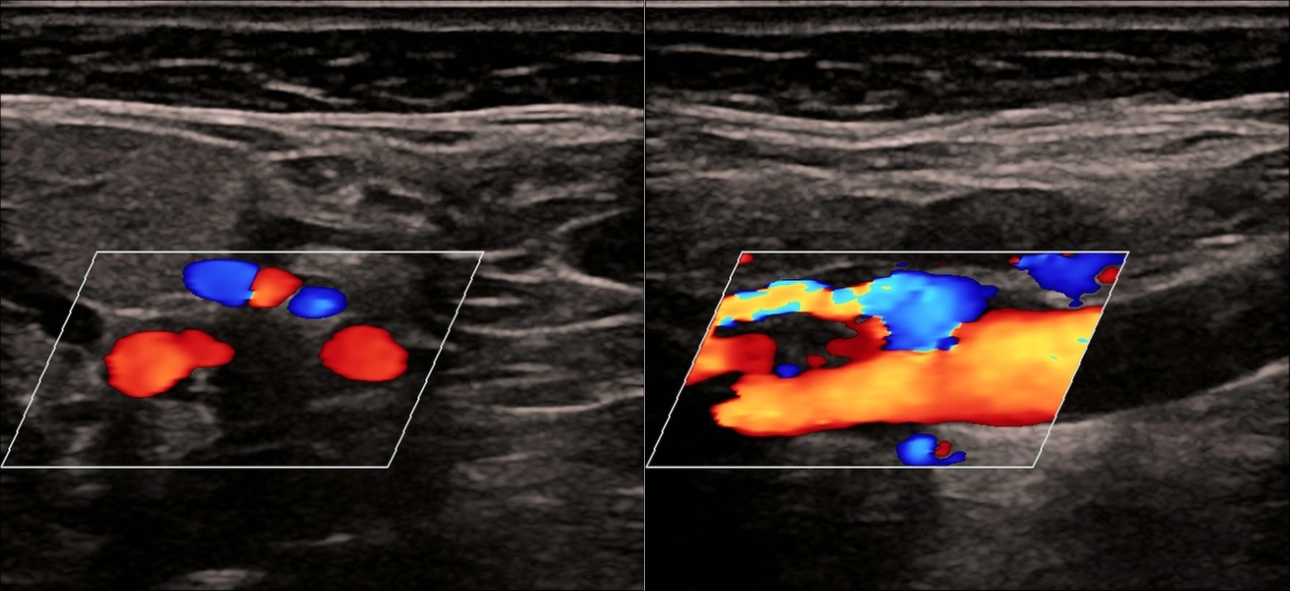
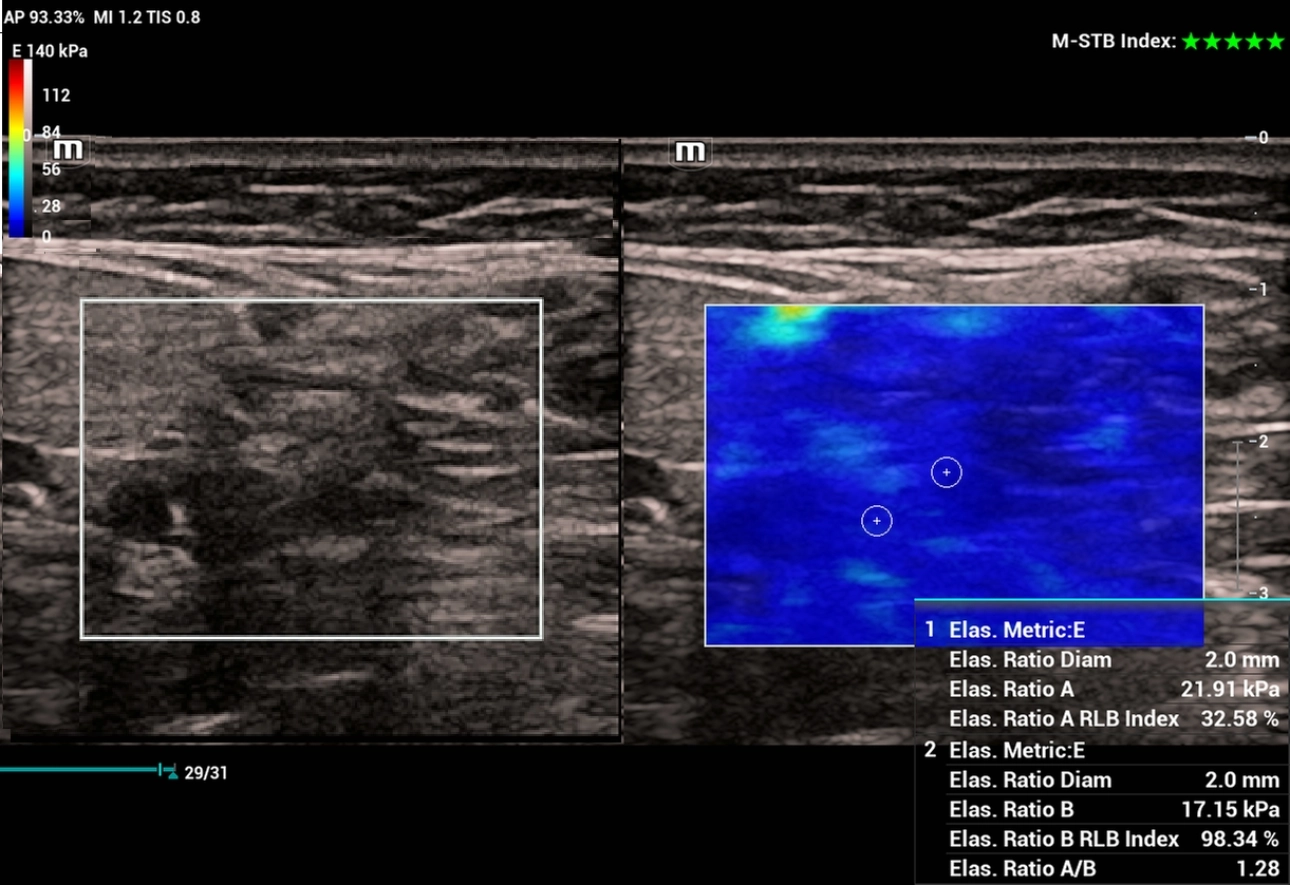
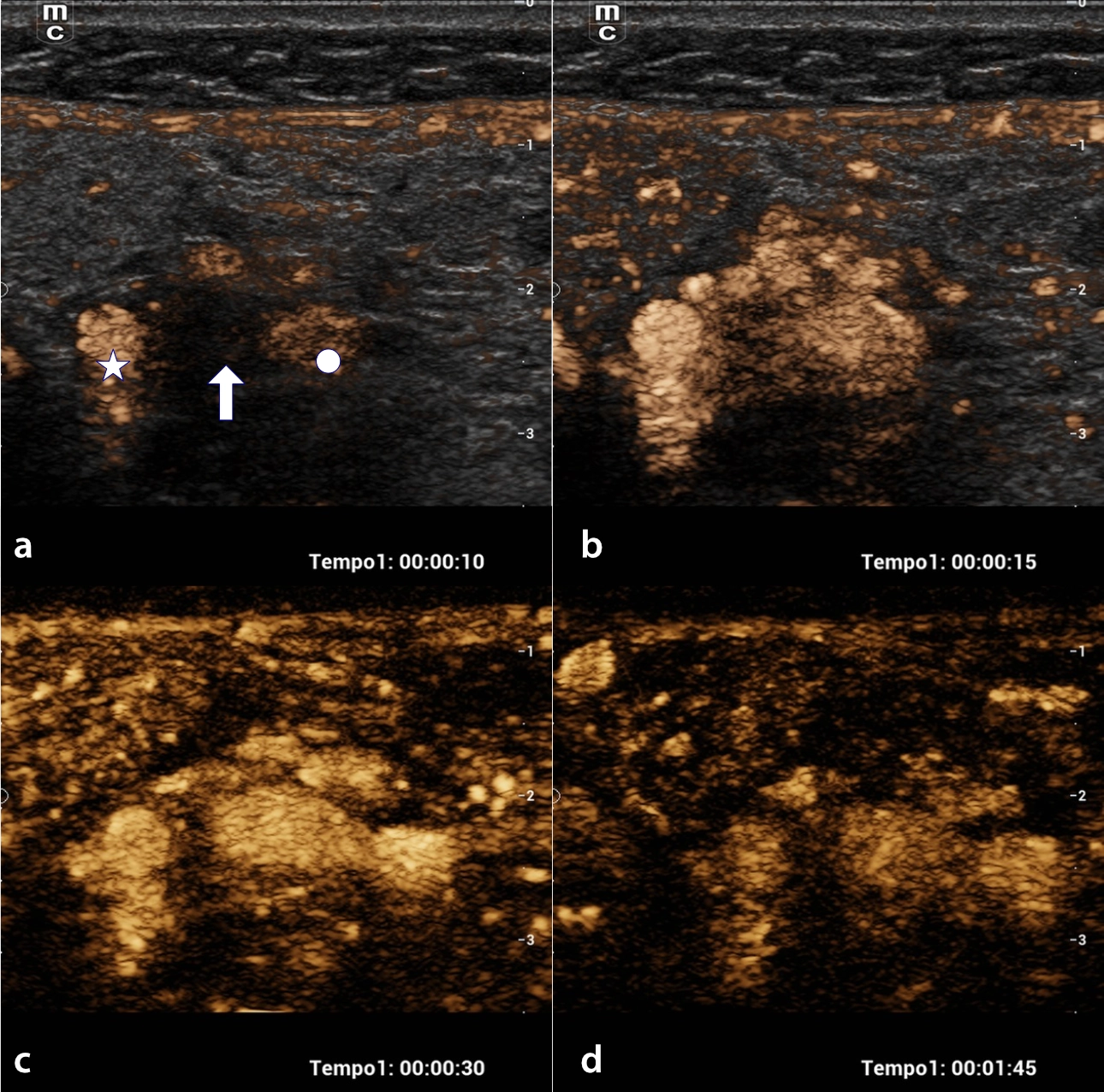
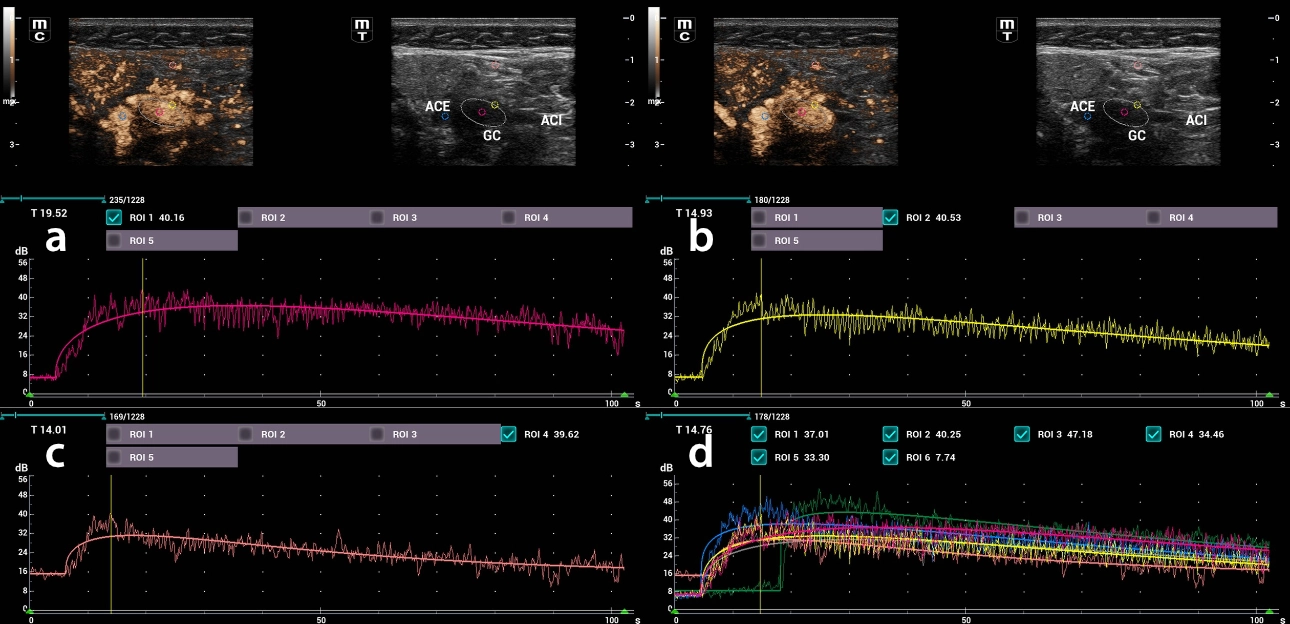
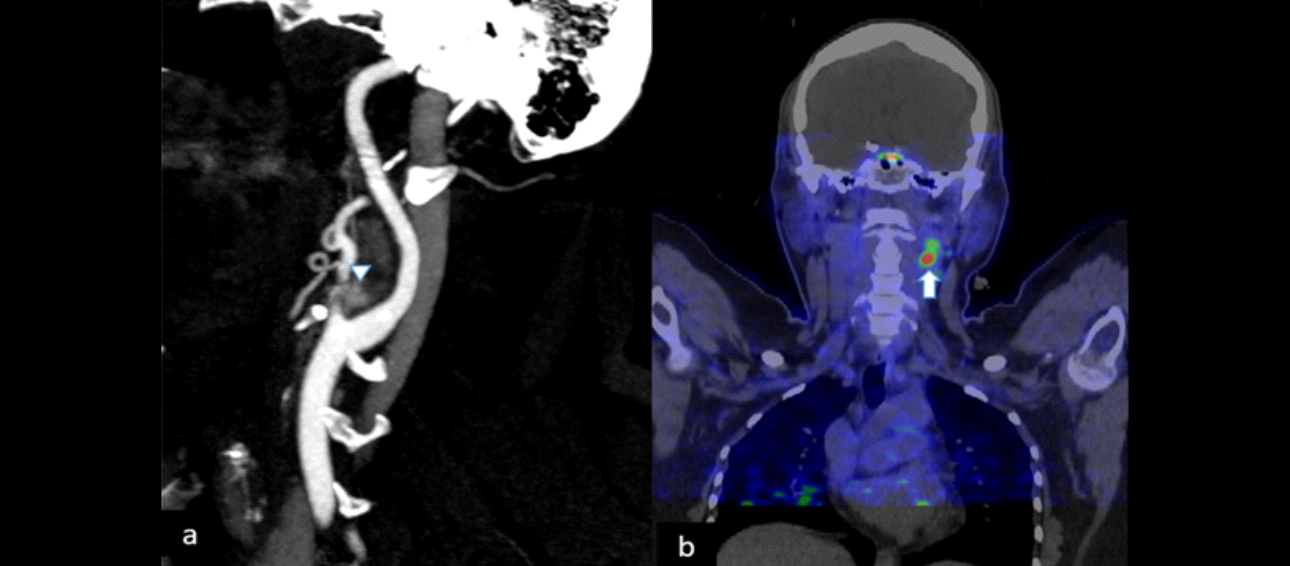
In a tomography study, a nodular lesion was observed, located at the level of the carotid bifurcation, of heterogeneous appearance, predominantly hypodense, showed enhance in the arterial phase and wash-out in the venous phase. The ultrasound, performed on Mindray Resona I9 system, showed a hypoechoic lesion, with defined edges at the level of the carotid bifurcation of 6.5 x 8.5 x 10 mm, with vascularity of peripheral predominance, with apparent feeding vessel at the expense of the external carotid artery (ECA) (Figure 1). Additionally, elastography and contrast ultrasound were performed. In elastography imaging with heterogeneous stiffness that fluctuated between 17 and 21 kPa (Figure 2). In contrast ultrasound, with sulfur hexafluoride, an initial enhancement pattern was observed in the arterial phase, reaching the maximum enhancement time between 14 and 19 seconds with an intensity of up to 40 dB and centripetal behavior (Figure 3 and 4). In the PET-CT study with 18 F-NOTA-OCTREOTIDE the lesion showed an increase in metabolism with radiotracer uptake with maximum SUV of 8.4 (Figure 5) as findings compatible with carotid glomus (CG)
Discussion
In the study of carotid paragangliomas, B-mode ultrasound and Doppler in its different modalities has shown high diagnostic performance, identifying up to 92% of these lesions with very particular characteristics of these tumors [1]. The main characteristics by ultrasound are its location at the bifurcation, defined edges, hypoechoic to heterogeneous lesions, highly vascularized [2]. In the case presented, in addition to complying with the epidemiological characteristics and the characteristic clinic of carotid paragangliomas, the typical pattern was shown by ultrasound when the lesion was found in the carotid bifurcation, increasing the opening angle between the internal and external carotid, however it was not highly vascularized with color Doppler, therefore, they were performed elastography and contrasted ultrasound. In the case of ultrasound elastography, there is no established parameter of the behavior of the carotid glomus, behaving heterogeneously. In some studies, a tendency to higher stiffness has been observed without establishing a specific quantitative value [3]. In our case the behavior was comparable, showing predominant areas of increased stiffness, from 17 to 21 kPa, this heterogeneous way of behaving could be explained by degenerative processes with a tendency to internal necrosis1. As for the contrast ultrasound in our case the lesion behave with the typical pattern of enhancement, characterized by a marked enhancement in the arterial phase, with a similar pattern to the adjacent carotid arteries and with wash-out in the venous phase3. Additionally, the diagnostic imaging in this case was complemented with multiphase tomography of the neck and PET CT with 18 F-NOTE- OCTREOTIDE showing itself as a tumor of attenuation in soft tissues, with arterial enhancement and with the typical location that presents important uptake to the radiotracer (octreotide) [4].
Conclusion
The use of multiparametric ultrasound is an ideal study method for the initial approach of carotid bifurcation paragangliomas and could be anadequate alternative for its complete characterization in patients in whom there is contraindication of the use of iodinated contrast. Adding information about the stiffness of the lesions with elastography and corroborating their vascularity, as well as the quantitative behavior of the enhancement by means of contrasted ultrasound could provide more information about the nature of these lesions. In future studies, the multiparametric study of the carotid glomus could provide more predictive information of its benign, malignant characteristics and that could even support its treatment and probable complications.
References
[1]. Demattè S, Di S arra D, Schiavi F, Casadei A, Opocher G. Role of ultrasound and color Doppler imaging in the detection of carotid paragangliomas. J Ultrasound. 2012 Sep;15(3):158-63. doi: 10.1016/j.jus.2012.05.001. Epub 2012 May 30. PMID: 23459221; PMCID: PMC3558042.
[2]. Delantoni A, Sarafopoulos A, Polanagnostaki A, Orhan K. B-mode and color Doppler imaging of carotid paragangliomas in different neck regions. J Ultrason. 2020 Nov;20(82):E218-e221. doi: 10.15557/JoU.2020.0037. Epub 2020 Sep 28. PMID: 33365160; PMCID: PMC7705482.
[3]. Pacini, P., Polti, G., Faggiano, A. et al. Multiparametric ultrasound evaluation of a case of bilateral carotid body tumor. J Ultrasound 24, 311–315 (2021). https://doi.org/10.1007/s40477-021-00581-zJournal of Ultrasound (2021) 24:311–315
[4]. Thelen, J., Bhatt, A.A. Multimodality imaging of paragangliomas of the head and neck. Insights Imaging 10, 29 (2019). https://doi.org/10.1186/s13244-019-0701-2
