


Clinical information
The patient was a 51-year-old male who had been suffering from a paroxysmal cough without any apparent cause for three months. He experienced occasional expectoration of a small amount of white sputum, with no symptoms such as hot flashes, night sweats, headaches, dizziness, or hemoptysis. He also reported occasional chest tightness, shortness of breath after physical exertion, and generalized weakness, but no palpitations. He occasionally experienced abdominal pain without any instances of diarrhea. Prior to this, the patient had no significant medical history.
The physical examination revealed the following: body temperature of 37.9 °C, pulse rate of 99 bpm, respiratory rate of 23 breaths per minute, and blood pressure of 132/65 mmHg. There were no signs of rash, jaundice in the skin or mucous membranes, or enlargement of subcervical lymph nodes.
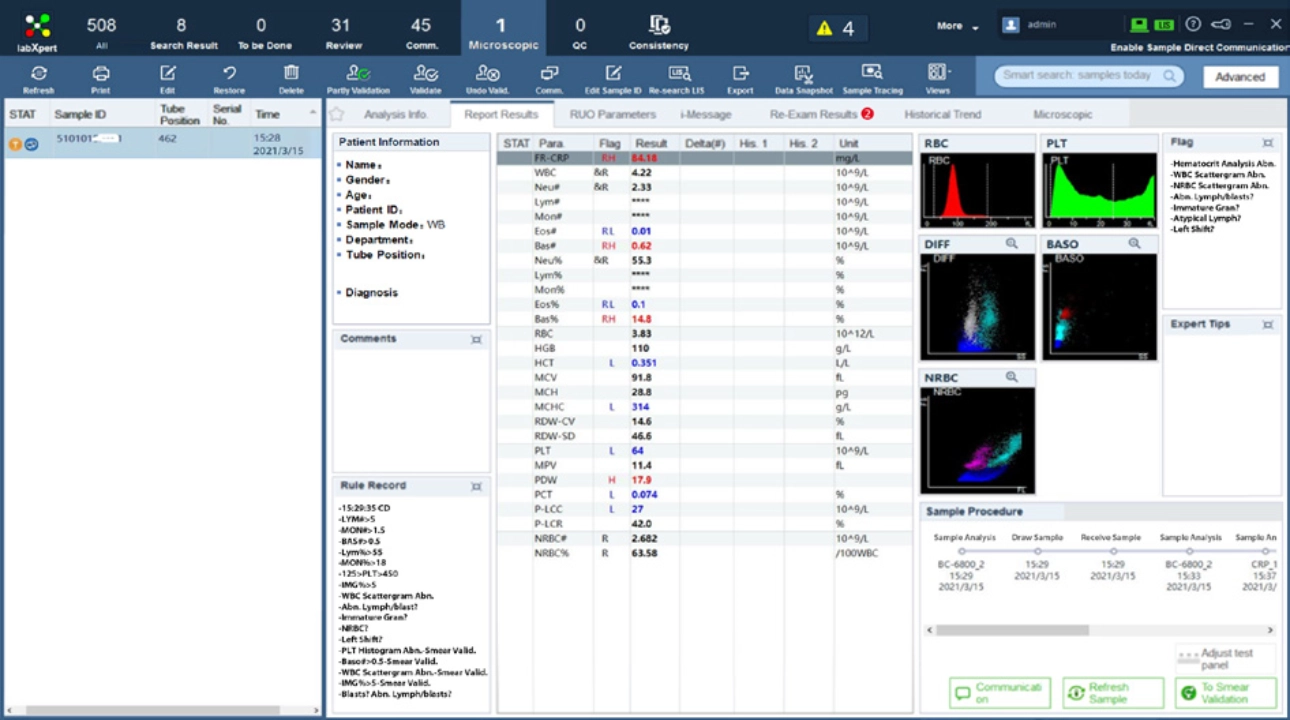
CBC results from Mindray BC-6800
WBC 4.22 × 109 /L ↓; RBC 3.83 × 1012/L ↓; HGB 110 g/L ↓; PLT 64 × 109 /L ↓; lymphocytes and monocytes could not be differentiated; the alarm of the instrument showed "WBC scattergram abnormal", "Nucleated red cells scattergram abnormal", and "Lymphocytes/blasts abnormal". A re-examination by microscopy was required. The results are shown in Figure 1.
Other laboratory test
HIV positive.
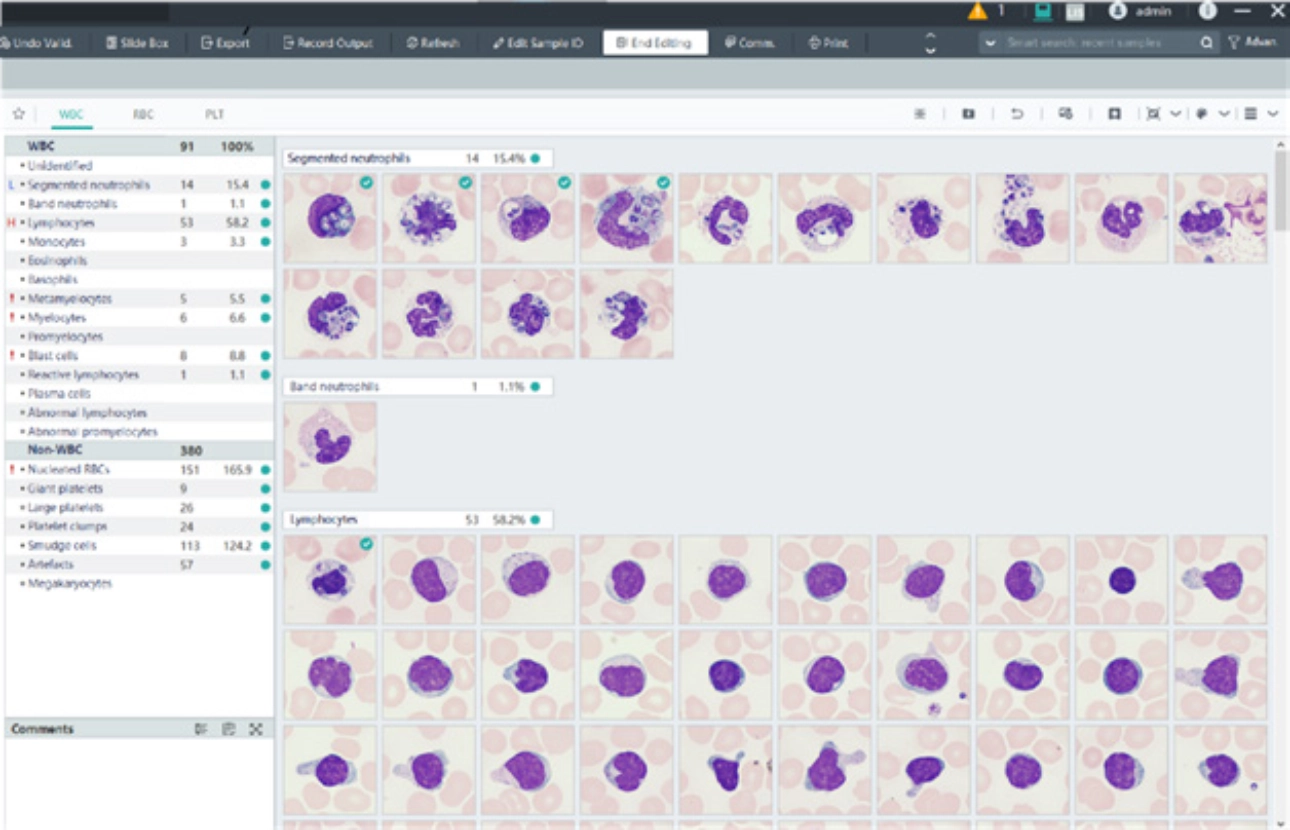
Examination of the peripheral blood morphology
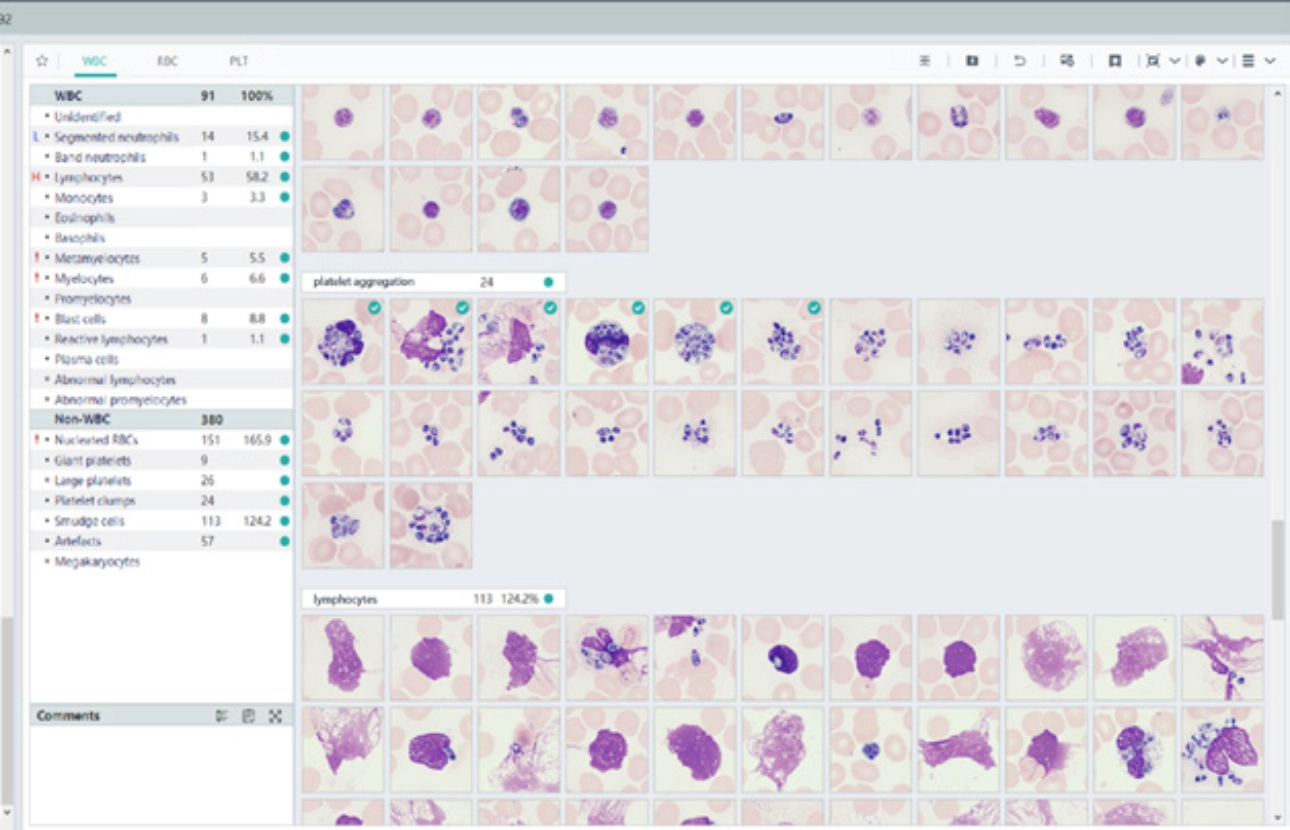
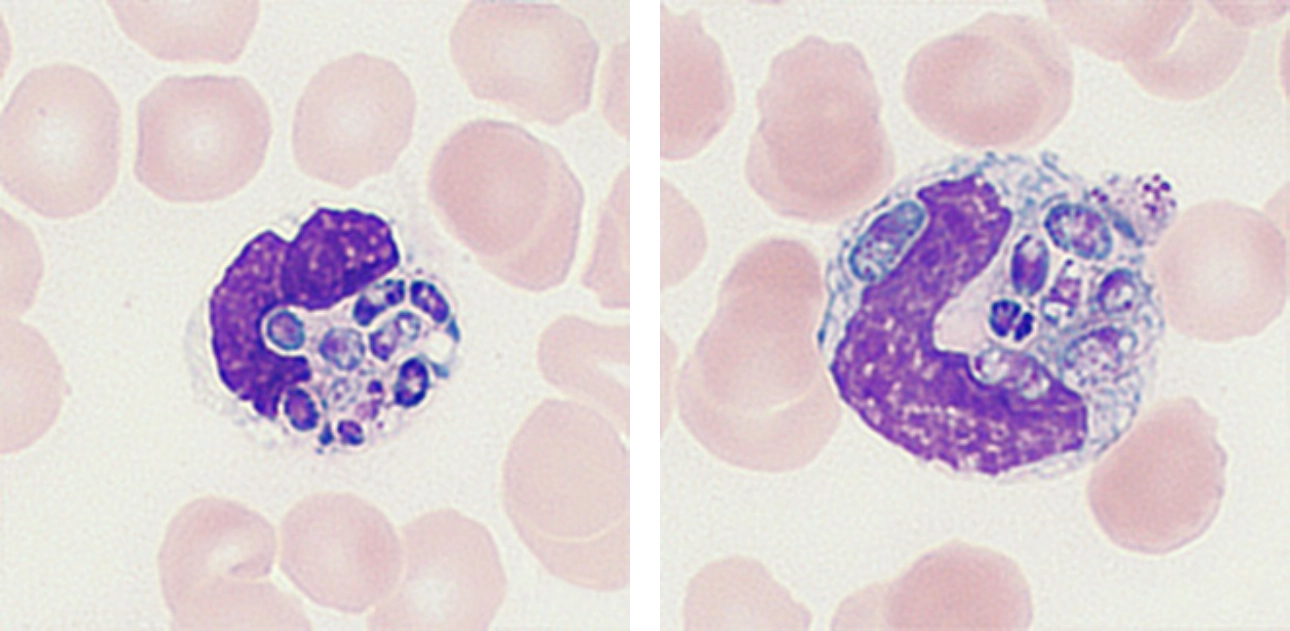
Yeast-like fungal spores were observed within the cytoplasm of some neutrophils, with the fungal cells having varying sizes and diverse morphologies (such as oval, elliptic, and sausage-shaped). Some fungal cells exhibited even thickness with two rounded ends, and a lightly stained diaphragm was visible in the middle. Scattered yeast-like fungal spores were also easily observed outside of the neutrophils.
Mature red blood cells varied in size, including elliptic, crenated, and a few teardrop-shaped and spherical forms. Additionally, schistocytes were observed.
Blood culture


Diagnosis
Talaromyces marneffei infection.
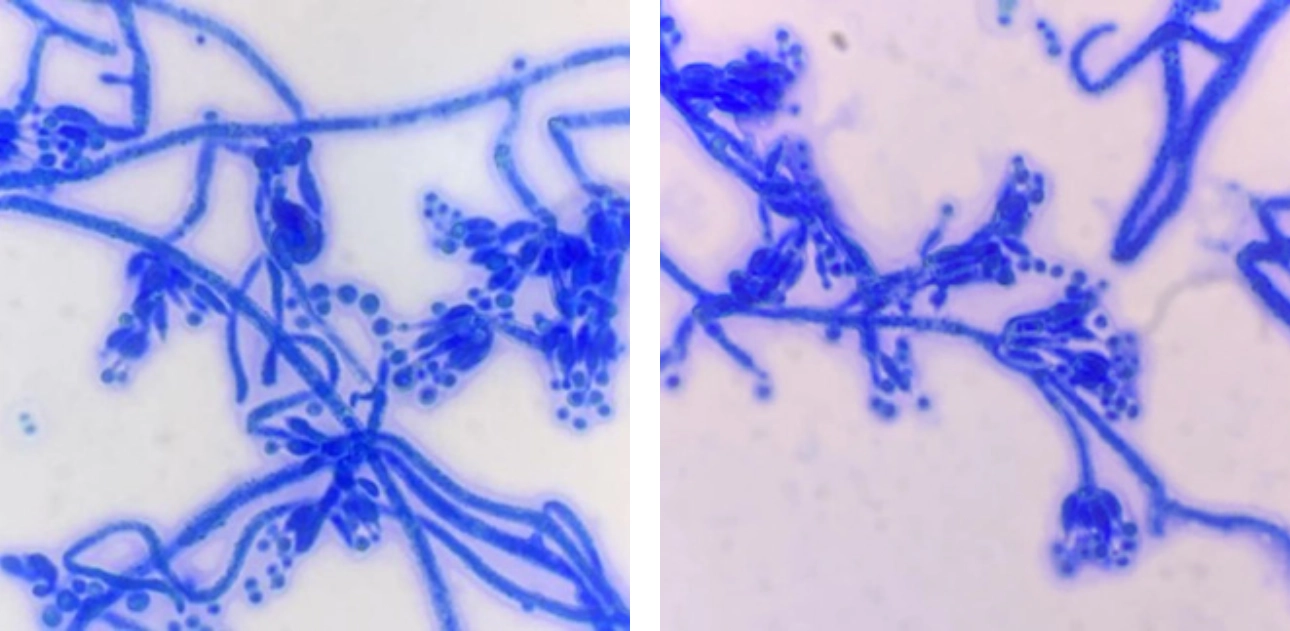
About Talaromyces marneffei infection
Talaromyces marneffei (TM) is the only known dimorphic fungus classified as Penicillium. It is a common opportunistic pathogen that causes secondary infections in patients with AIDS and malignancies, as well as the immunocompromised. TM is endemic in Southern China and Southeast Asia. It invades the respiratory system and then spreads throughout the body via blood circulation. The clinical manifestations of TM infection are complex and can affect various organs such as the lungs, liver, spleen, and skin, leading to a considerably high mortality rate.
The disease is classified into localized and disseminated infections according to the location and characteristics of the lesion. Most AIDS patients with concomitant TM suffer from disseminated TM infections. Routine examination indicators for these patients are non-specific, making the diagnosis reliant on both clinical manifestations and etiology.
Case analysis
The re-examination of the peripheral blood smear in this case revealed that neutrophils were engaging in phagocytosis of yeast-like fungal spores, as detected by the MC-80 Automated Digital Cell Morphology Analyzer. This finding suggested a "highly suspected HIV with TM infection" diagnosis and necessitated immediate communication with the clinical departments. A blood culture was performed upon the patient's hospital admission, and after 17 hours, an alarm was triggered from the aerobic bottle. Microscopic examination of the blood smear revealed the presence of fungal spores, which were then transferred to Sabouraud agar plates for culturing at 25 °C and 37 °C, respectively. The diagnosis of TM was confirmed through mass spectrometry analysis.
The utilization of an automated hematology analysis line, along with an intelligent automated digital morphology analyzer, follows the laboratory's retesting rules and enhances the efficiency and accuracy of hematology testing. During the first routine blood test of this patient, the BC-6800 system triggered an alarm due to abnormalities observed in the scattergram. Additionally, fungal spores were detected through smear reading using the MC-80 analyzer. These findings collectively provided a basis for the early diagnosis and treatment of the disease, contributing to a reduced mortality rate.

Call for case studies
- Do you want to share your case with us? We will share your case in the upcoming issues with acknowledgement.
- IVD Cases: You are recommended to submit any typical, misdiagnosed, special or rare cases that received a definite diagnosis or successful treatment. Cases that involved effective communication between the laboratory and clinical departments are particularly encouraged.
- Format: You are required to include four sections in your entry: "Case Introduction, Case Details, Case Analysis, and an Executive Summary". The Case Details section must include: primary medical history, positive/negative test results that aided in the diagnosis, and the diagnosis and treatment process.
- Please submit your entry in a Word document (in English) by sending it to hoishan.kwok@mindray.com by August 30th, 2023.
- The email should come in a subject that reads: country+name of the entry + name of the applicant.

