Ultrasound Journal 18 - Multiparametric Approach in Ultrasound Diagnosis of Metabolically Associated Fatty Liver Disease
By Venidiktova D.Yu., Borsukov A.V. [1] 2023-09-25

Introduction
A 57-year-old female patient was admitted to the admission department of a multidisciplinary hospital with the preliminary diagnosis "acute exacerbation of chronic acalculous cholecystitis". Past medical history of weight gain over the past 9 years after accidental detection of diabetes mellitus type 2, for which the patient takes blood glucose-lowering drugs. Her blood pressure rose to 140-150/90 mm Hg, for which she occasionally had headaches. Complaints of general weakness, pain in the right subcostal area during the last two months, nausea, thirst, absence of appetite.
Clinical and laboratory findings
Objectively: body mass index (BMI) 30.8 kg/m2, waist circumference (WC) 111 cm, hip circumference (HC) 109 cm. Abdomen was soft and painful upon palpation in the right subcostal area and epigastrium. The liver protrudes from under the edge of the rib arch by 1 cm.
General blood and urine tests: leukocytosis 10.4 × 109/L, other parameters within normal limits. The patient was admitted to the gastroenterological department for further examination and treatment.
Hepatitis C and B viruses and HIV infection were not found.
Biochemical blood tests: total protein 67 g/L, total bilirubin 20 µmol/L, direct bilirubin 3.9 µmol/L, ALT 39 U/L, AST 34 U/L, ALP 115 U/L, GGT 39 U/L, glucose 6.1 mmol/L.
Questionnaires
CAGE (Cut-annoyed-Guilty-Eye) Chronic Alcohol Intoxication Assessment Questionnaire - 0 points.
AUDIT (The Alcohol Use Disorders Identification Test) to identify alcohol use disorders - 0 points.
DEBQ (Dutch Eating Behavior Questionnaire) to assess the type of eating disorder - restrictive type of eating disorder.
IPAQ (International Questionnaire on Physical Activity) - 14 points (hypodynamic).
IPAQ (International Questionnaire on Physical Activity) - 62 points (moderate motor activity).
Compliance Level Questionnaire - 76 points (average level of compliance).
B-mode and Color Flow Doppler (CFD)
Conclusion of the ultrasonic liver examination in B-mode: increased size of the liver, diffuse changes of liver parenchyma (like liver steatosis) - increased echogenicity, decreased conductivity, heterogeneous content of gall bladder (wall-thick bile), local thickening of gall bladder wall up to 5 mm, meteorism. In CFD, the number of vascular loci per unit area was not changed. Visceral obesity (S>30 mm).
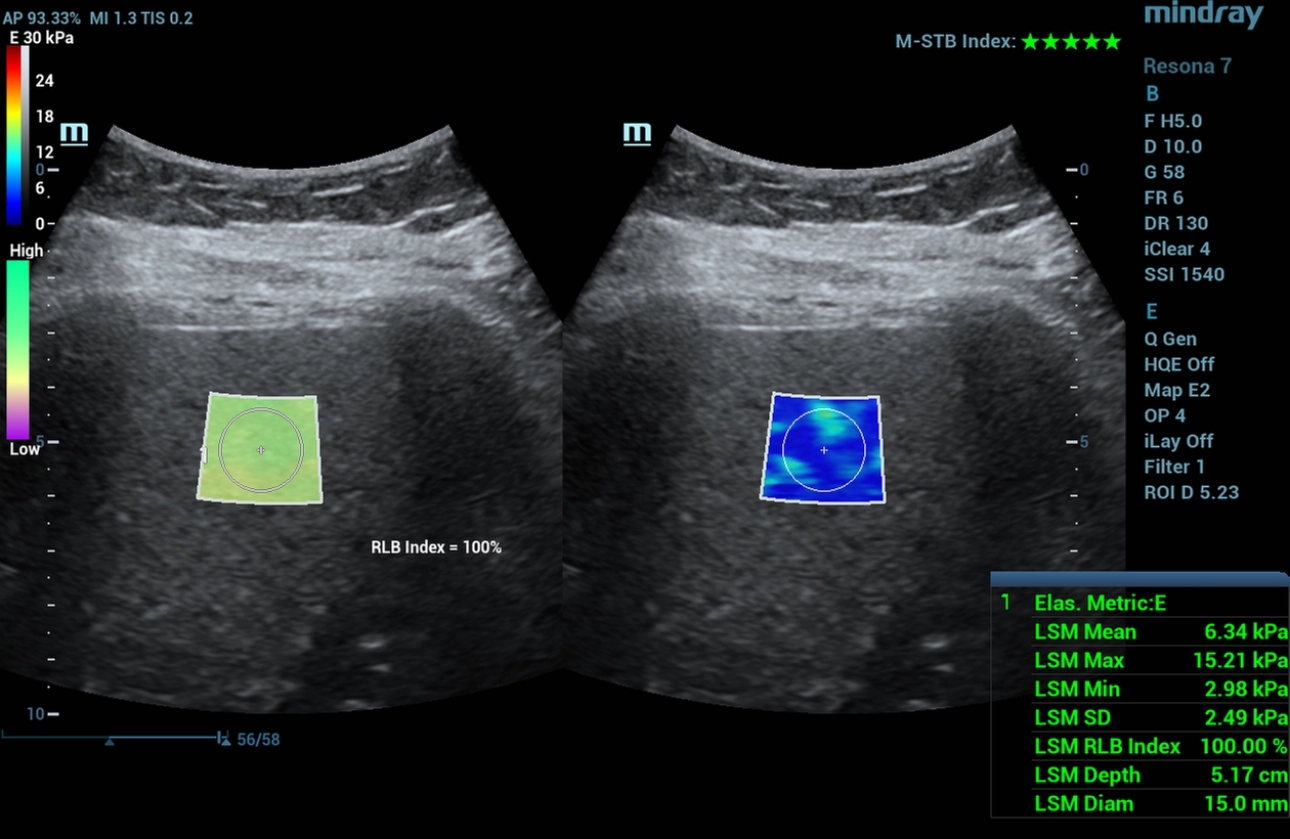
Two-dimensional shear wave elastography (2D-SWE, STE)
Two-dimensional shear wave elastography values correspond to F0-F1 stage of the fibrotic process - stiffness 6.34 kPa - clinically insignificant liver fibrosis (Figure 1).
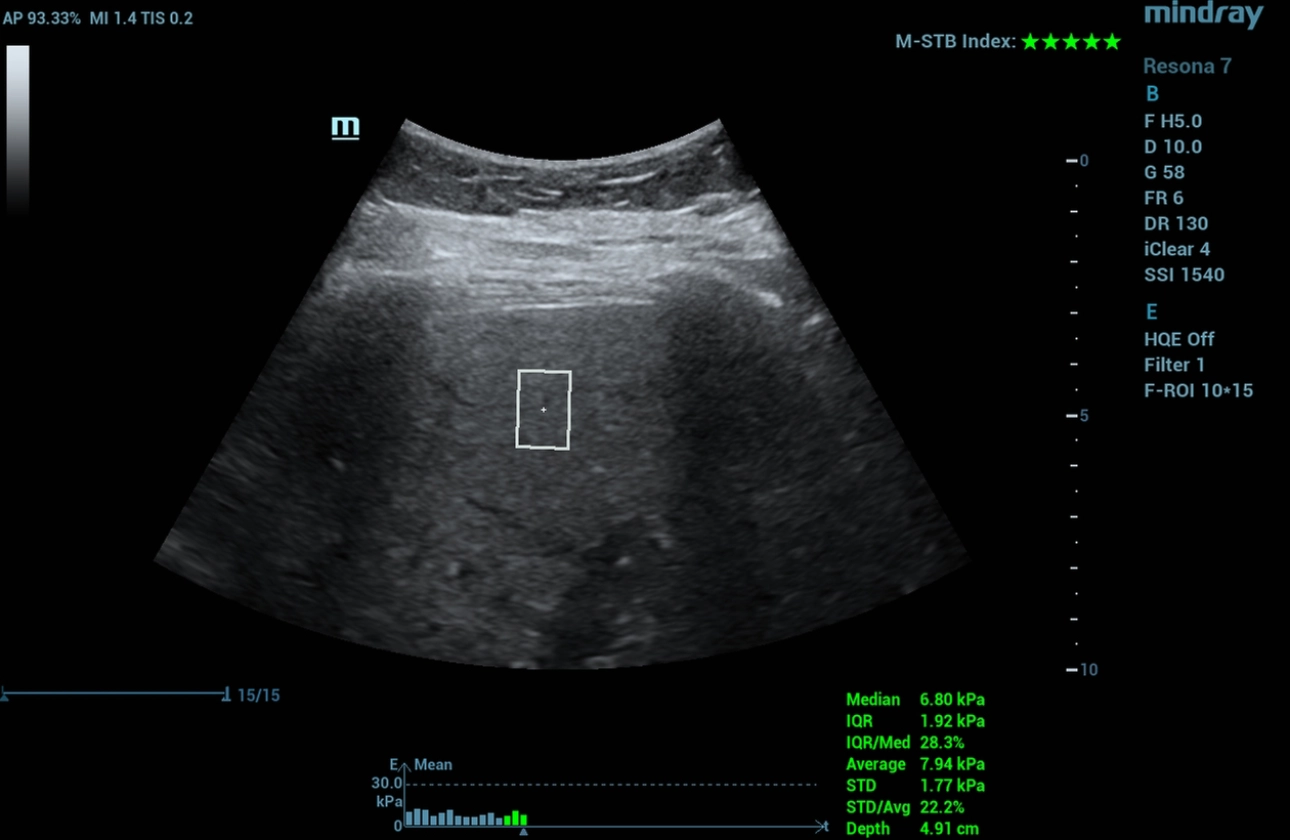
Point shear wave elastography (pSWE, STQ)
Shear wave point elastography values correspond to F0-F1 stage of fibrotic process - stiffness 6.8 kPa - clinically insignificant liver fibrosis (Fig. 2).
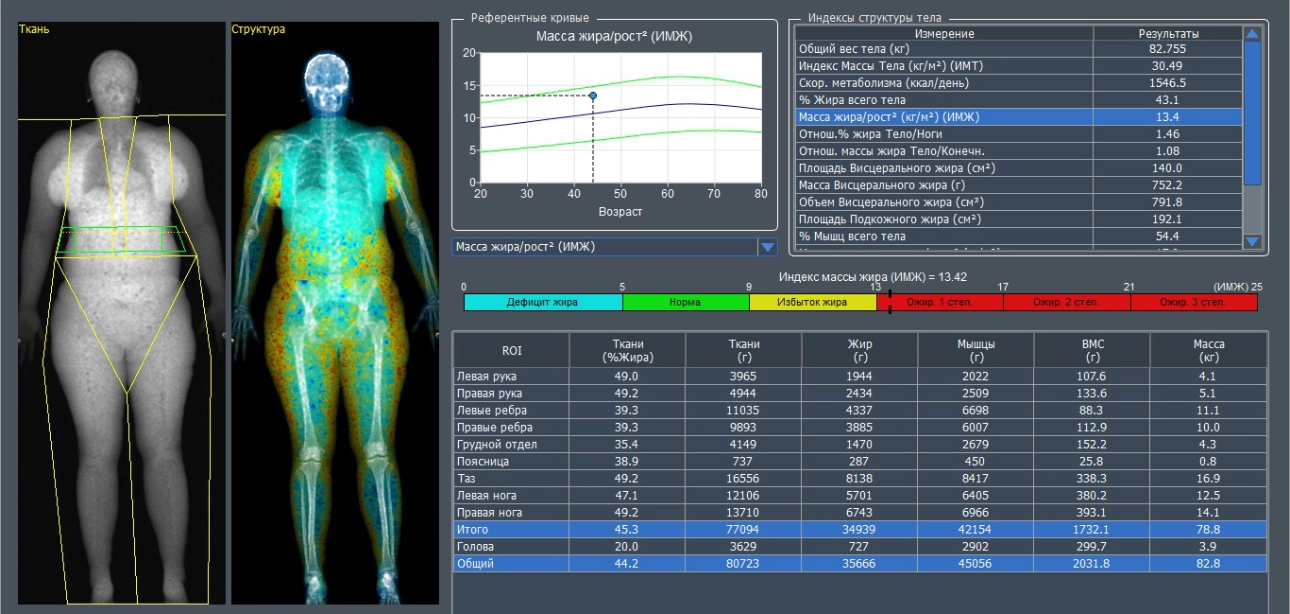
Dual-energy X-ray absorptiometry (DEXA)
Given that the patient refused liver biopsy for subsequent evaluation of histological micrographs according to SAF and NAS scales, dual-energy X-ray absorptiometry in "Whole body" mode was performed as a reference method to assess visceral obesity, risk factors of metabolic syndrome: percent adipose tissue 43.1%, fat mass index 13.42 (degree I obesity), visceral fat area 140 cm2 (Fig. 3).
Discussion
Clinical and laboratory data
Evidence of comorbid pathology on the background of obesity with diabetes mellitus, arterial hypertension, fatty liver disease.
B - regimen, Doppler sonography
Ultrasound signs of diffuse liver changes of steatosis type due to increased echogenicity and decreased sound conductivity of the signal, visceral obesity was detected.
Elastography
Two-dimensional and spot shear wave elastography modes determined clinically insignificant liver fibrosis (F0-F1).
Diagnosis
Based on the results of clinical and laboratory and instrumental methods of investigation, the diagnosis was added: "Chronic acalculous cholecystitis at the acute stage. Sugar Type 2 diabetes. Metabolic associated fatty liver disease, steatosis stage. Grade I Obesity."
Key points
Use of multiparametric ultrasonography in a comprehensive diagnostic algorithm in patients with obese metabolically associated fatty liver disease can be used for diagnosis and monitoring of diffuse changes.
[1] Problem Research Laboratory "Diagnostic Studies and Minimally Invasive Technologies", Federal State Budgetary Educational Institution of Higher Professional Education Smolensk State Medical University, Ministry of Health of Russia
