


In Mindray’s Case Observation section, you will find “comrades in arms” who encounter similar problems with you; hear different fresh diagnosis and treatment ideas and solutions; learn more comprehensive and intelligent monitoring methods and analysis methods; find more efficient and applicable clinical decision-making experience.
Cardiac arrest has become an important health issue of public concern worldwide. Since 2010, the American Heart Association (AHA) Guidelines for Cardiopulmonary Resuscitation have continuously increased the priority of chest compression and proposed the concept of high-quality cardiopulmonary resuscitation based on high-quality chest compression. It has been clinically proven that the guarantee of high-quality chest compressions is inseparable from real-time monitoring feedback.
In 2020, the update of the AHA Guidelines for Cardiopulmonary Resuscitation clearly recommends monitoring feedback to be performed during cardiopulmonary resuscitation to optimize the quality of cardiopulmonary resuscitation and improve patient prognosis. The current measures used to monitor the quality of cardiopulmonary resuscitation mainly include invasive blood pressure monitoring (IBP), central venous oxygen saturation (ScvO2), partial pressure of end-tidal carbon dioxide (PetCO2) and cardiac ultrasound. However, due to the limitations such as large trauma, expensive consumables, time-consuming and complex procedures, the clinical availability of the above monitoring techniques has been reduced, and their current application in the process of cardiopulmonary resuscitation is not extensive enough.
Studies have found that pulse oximeter waveforms based on photoplethysmography signals can reflect the blood volume status of patients, and it is non-invasive, easy to obtain, and real-time.
In 2011, Mindray cooperated with Peking Union Medical College Hospital based on this technical principle. Through animal experiments, normal population experiments, human clinical trial and clinical validation trial, Mindray finally innovatively developed the cardiopulmonary resuscitation quality index (CPR Quality Index, CQI). When CQI <60, it means that the quality of cardiopulmonary resuscitation is poor, and the patient has a low probability of Return of Spontaneous Circulation(ROSC); when CQI ≥60, it means that the quality of cardiopulmonary resuscitation is good, and the patient has a high probability of ROSC. A multicenter study confirmed that CQI’s performance in judging the quality of resuscitation and the patient’s probability of ROSC is non-inferior to the partial pressure of end-tidal carbon dioxide.
Let’s take a look at a clinical case.
Case Introduction
A 71-year-old male patient suffered a sudden cardiac arrest outside the hospital.
Treatment
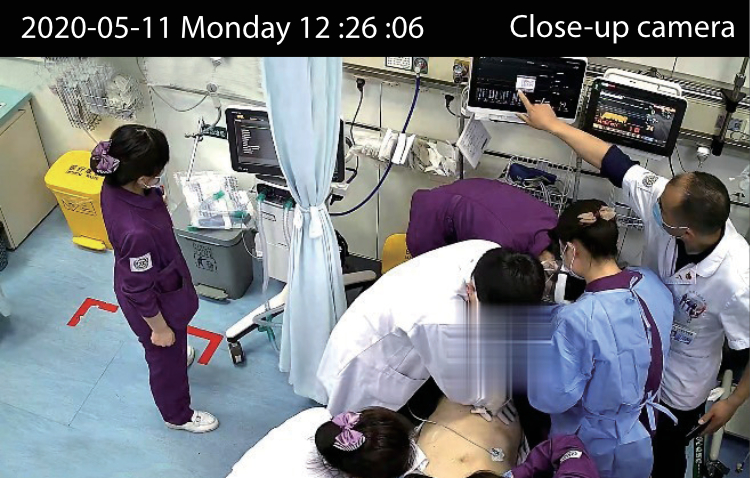
After the patient was sent to the emergency department, the rescue team immediately implemented standard chest compressions on the patient, and the other team members performed tracheal intubation at the same time, and venous access was establishment.

After starting compression, the clinical staff entered the “rescue mode” by clicking the shortcut key on the monitor screen. In this mode, all physiological alarms of the monitor were blocked. At the same time, clinical staff connected the pulse oximeter probe to obtain CQI parameters.
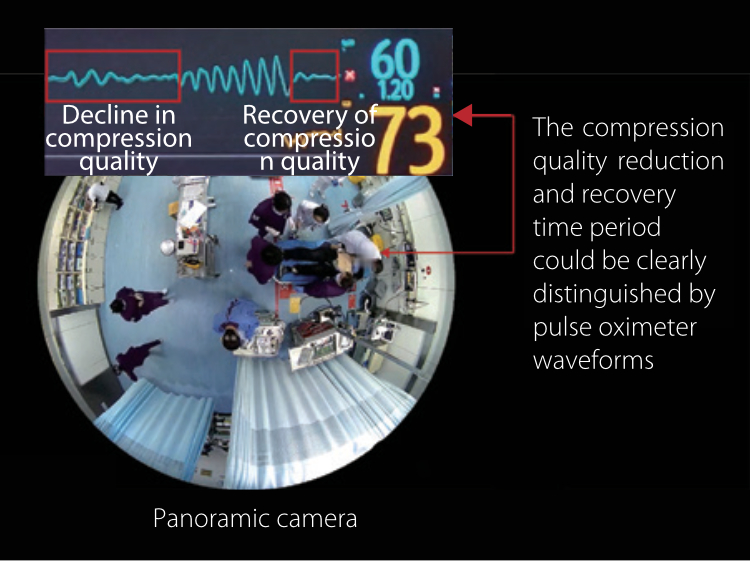
Due to the high quality compressions and the good general status of the patient, the patient’s pulse oximeter waveform was regular and had obvious peak groups, which proved that the patient’s peripheral perfusion state was good. Therefore, the CQI parameter value was relatively high and the initial value was 80.
During the compression process, the rescuer periodically observed the monitor check the patient’s status. At this time, the compression quality decreased due to distraction. It can be seen that the amplitude of the pulse oximeter waveform decreased significantly which means that the patient’s perfusion state was lower than before, and the CQI parameter value also decreased to 70. The rescuer discovered this situation in time and immediately improved the compression intensity, after which the CQI parameter value increased.
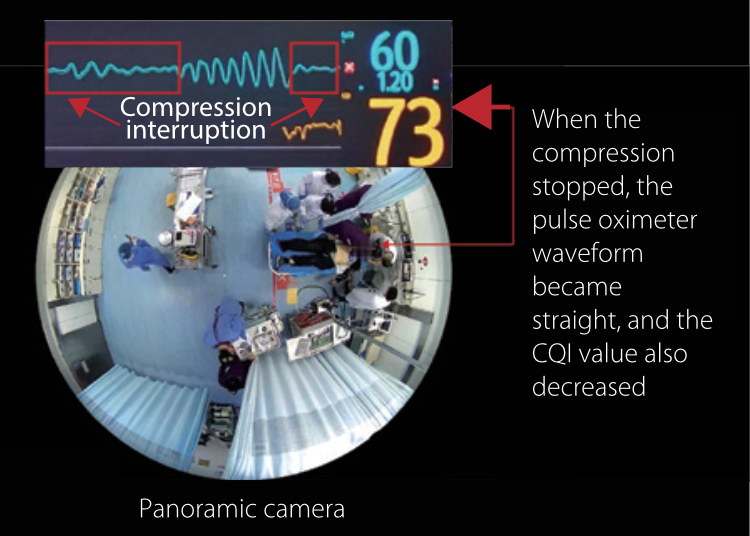
According to the “Chinese Expert Consensus on Cardiopulmonary Resuscitation”, in order to ensure the quality of chest compression, the personnel performing compressions must be replaced every 2mins. When changing personnel, the compressions would inevitably be interrupted for a short time. When the compressions were interrupted, the patient had no blood perfusion. Therefore, the guidelines also require that the interruption time of the compressions be less than 10s. During the changing of personnel performing compressions, the patient’s pulse oximeter waveform became a straight line when compressions were interrupted, indicating that the patient’s perfusion stopped at this time. Meanwhile, the CQI parameter value also decreased very sensitively, from 84 to 73 within a few seconds. When the compression was restarted, the patient’s pulse oximeter waveform showed a regular compression waveform, and the CQI value also rose.
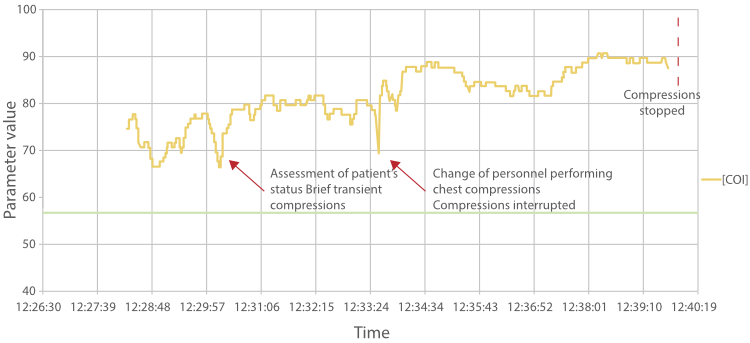
After a 12-minute rescue process, the medical staff adjusted the compression strategy in a timely manner under the guidance of the CQI to ensure high-quality compressions, and gave other resuscitation measures in accordance with the guidelines and expert consensus. In the end, the patient was successfully rescued, and ROSC was observed.
Summary
The patient's CQI parameter value changes throughout the rescue process. The CQI has always remained above 60, and the overall trend is increasing, indicating that the compression quality is high and the patient's perfusion status is continuously improving. When the compression quality is reduced, the CQI can respond quickly, and remind the rescuer through the parameter value change, so as to win more opportunities to rescue the patient's life.
References
1. Panchal A R, Bartos J A, Cabañas J G, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care[J]. Circulation, 2020, 142(16_Suppl_2): S366-S468.
2. Shao, F., Li, C. S., Liang, L. R., Li, D., & Ma, S. K. (2014). Outcome of out-of-hospital cardiac arrests in Beijing, China. Resuscitation, 85(11), 1411–1417.
3. Mau MK, Yamasato KS, Yamamoto LG. Normal oxygen saturation values in pediatric patients[J]. Hawaii Med J, 2005, 64(2):42, 44-45.
4. Salyer JW. Neonatal and pediatric pulse oximetry[J]. ResPIr Care, 2003, 48(4):386-396,397-398.
5. Medical Device Clinical Trial Report-CPR Quality Index (CQI) Clinical Trial